The first month of the new year and the first challenge. Monday is the big day for me. In the essence, my grant application was shortlisted for the interview where I have to face the challenge and prove that I worth it.
Anyone for a challenge?
The proposed application seeks to go to the US lab and gain an expertise in an interdisciplinary methodology to monitor and capture the dynamic of cancer spread (metastasis) in real time. This experimental approach would accelerate our understanding of neuroblastoma metastasis which is one of the reasons for failure in the treatment of neuroblastoma. If we know how neuroblastoma cells spread, then we can find the weaknesses in the process and create new drugs or use existing to target it.
I feel that sharing my worries with you makes me stronger. I am looking forward to this challenge with my head up and hope to feel your support at this crucial moment.
When I look back on my journey in 2017, there were many junctions, traffic lights and stops as well as ups and downs. Junctions were to make decisions, while traffic lights and stops – to be patient. Ups and downs were my feelings of satisfaction. The good mix of both kept me to stay human. It is not the number of grants received that matters it is who around you. I have met genuinely curiosity-driven students who made this journey fascinating and very special.
My most memorable Ups were the successful examination and graduation of my PhD student John Nolan, organisation and chairing the IACR Meeting session: Challenges in Childhood Cancers, the Mad Hatter’s Tea Party and the Gala Dinner with the CFNCRF, the launch of my very own research team thanks to the funding by the NCRC and the Neuroblastoma UK, the successful completion of two final year undergraduate and two MSc projects, and welcoming the new PhD student Tom Frawley.
My team is growing and I am looking forward to 2018!
The researcher’s path includes days when you feel so low because your grant or paper was rejected or even both within a very short time frame. It happened to me a couple of weeks ago. At this point, I felt helpless sarcastic and non-motivative reading reviewer’s comments. One reviewer mixed up neuroblastoma with a brain tumour, so their comments were not relevant. Another just found no time to read through, the sentence was very short – ‘not a priority or interest‘. One more went to their area of expertise asking to fulfil it rather than comment on the actual focus of the study. Such comments are so common that any submission of results or a proposal could be considered as a draw. It has been neither my first time not the last. More to come.
On November 20th, the Irish neuroblastoma researchers have met for the first time to set up a collaborative research hub. The aim is to consolidate their expertise and skills in order to crack the neuroblastoma code together.
They all have different science background spanning from molecular and cellular biologists, immunologists, tissue-engineering, bioinformatics, mathematical modelling and clinicians representing RCSI, UCD, TCD, OLCHC and NCRC. During this meeting, researchers talked about their challenges and progress finding out that we are complementing each other projects. Clinicians from different OLCHC departments exposed basic researchers to realities of the disease. None would find this information in academic papers: it is what you see in the clinic and how it works in practice.
Big thank you to Dr Cormac Owens for the invitation and linking us together and Prof Jacinta Kelly for mapping the support available from the NCRC and CMRF.
Our next meeting will be held in RCSI in January 2018.
Happy Birthday the Irish Neuroblastoma Research Consortium!
As a part of Science Week, our Department hosted Lab Safari for the secondary school students aiming to give a sense of what scientists do in the lab. The focus of my research is the identification of novel biomarkers for neuroblastoma response to chemotherapy. So, we decided to explain the concept of biomarkers and the importance of discovering novel biomarkers for neuroblastoma. Between me and John we covered biomarker’s basics and carried out the detection of MYCN in neuroblastoma cell lines. Here, I am summing up our activities in the form of Qs & As:
1. What are biomarkers?
Biomarkers are signposts of the body condition. Biomarkers – bio is for biological and markers – for molecules indicating that something is going wrong or differently in the body. They can help doctors to read these changes and identify a condition or disease. There are biomarkers for heart disease, cancer, diabetes and many others.
2. What type of molecules can serve as biomarkers?
Various types of molecules can do the job as long as they can differentiate the normal and abnormal process in the body. It can be DNA, RNA, proteins and hormones. These molecules can be detected in the blood, urine, stool, tumour tissue or any other bodily tissues or fluids.
3. How can we discover novel biomarkers?
Research, research and again research. We have to learn more basic facts about DNA, RNA and proteins. We need to be able to link this knowledge with health conditions including cancer. We need to identify how these molecules speak about the unhealthy conditions. We need to explore whether biomarkers exist within the disease that can predict the response to treatment and outlook.
4. What biomarkers are known in neuroblastoma?
There are various biomarkers that are specific for neuroblastoma. Catecholamines in urine are chemicals produced by neuroblastoma cells. Chromogranin A – is a protein that can be detected in the blood. It is unspecific biomarker because it can be secreted by neuroblastomas and some other tumours (e.g. pancreas and prostate cancer). Various chromosomal aberrations can be biomarkers of neuroblastoma aggressiveness. One of the strongest predictors of rapid neuroblastoma progression is MYCN status.
5. What is MYCN?
The MYCN is a proto-oncogene protein and a member of the MYC family of transcription factors. MYCN was identified in 1983 and very soon became a routine biomarker for neuroblastoma aggressiveness. This protein is very important for the normal embryo development. The amplification of this gene leads to the excess of MYCN protein in cells prompting cells to grow and divide faster transforming normal cells into tumour cells.
6. How did we detect MYCN in neuroblastoma cell lines?
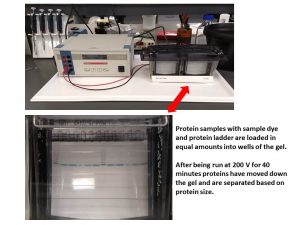
A day before the demonstration, we carried out some preparation steps. We selected several neuroblastoma cell lines with known MYCN status. Some cell lines had MYCN amplification, other didn’t. Among those that did have the amplification, the expression of MYCN protein was different giving us a good illustration of biomarker’s quantity. So, we run SDS-PAGE, a technique that helps to separate the cellular protein mix based on their size.
Then the separated proteins were transferred onto a membrane and exposed to a buffer containing an antibody for MYCN (primary antibody). This antibody recognises only MYCN. At the next step, we added another antibody that has a dual role – it can attach to the primary antibody and produce a signal that can be visualised. The next step would have been the visualisation itself and the one for Lab Safari. So, we were ready.
Once we finished the basics of biomarkers, we moved to the biomarker MYCN detection step. The buffer for visualisation was added and the membrane was imaged.
John’s Master Class
If you like this idea and want to have this demonstration for your science classes at school, please contact me and we would be happy to do it for you.
This network of galaxies is a new project to get insights on how and where childhood cancer is placed on social media. It is a collaborative project with Prof Richard Arnett. It is already very exciting and more to come!
#ChildhoodCancerAwarenessMonth is over. However, childhood cancer is not going away. The battle is not over. Families will be still affected by the lack of treatment options available to their child. More research is needed. Please do support enthusiastic people who do want to make the change. Every single contribution counts.
Scientist as imagined by a 7-year-old boy
The more important reason is that the research itself provides an important long-run perspective on the issues that we face on a day-to-day basis. (Ben Bernanke)
I would like to thank everyone who followed my blog during this month and hope would continue!
We hear great news from the US labs that a new treatment is on the way for children with cancer. Most of their research is funded by charities and success stories appear because of the people who want to make dreams come true for kids with cancer and their families. Dreams for longer and healthier life.
Interestingly, the study led by Professor Bernie Hannigan, the University of Ulster, which was published by Medical Research Charities Group, identified main gaps that keep Ireland at the bay:
Childhood cancer research areas are not prioritised, including neuroblastoma.
No Government funding support for childhood cancer research. The research has to compete on general terms with well-funded research groups/centres/clusters focused on the adult cancers (breast, prostate, etc)
No systematic involvement in research of Patients or other lay people.
No medical research charities to fill the gap in childhood cancer research funding.
In preparation for ‘Discovery’ Launch Night-An Exploration of Cancer Research Through Art, the event that took place on Tuesday at The Tara Building. Tara Street, D2.
Things that are absolutely ordinary for researchers become inspirational! I was glad to be able to provide such environment.
Continuing the fundraising theme, I would like to introduce The Conor Foley Neuroblastoma Cancer Research Foundation. It is founded by the family aiming to raise awareness and funding for neuroblastoma – one of the most aggressive childhood cancer. This charity is being driven by parents who lost their son to neuroblastoma. They want to fill this gap as well as bring attention to the lack of funding for childhood cancer research.
Their son Conor was diagnosed with neuroblastoma at the age of four. He was a teenager when he relapsed. He had been 10 years cancer-free. After all possible treatments, neuroblastoma took over.
His mom Margaret says:
“We always dealt with Conor’s illness privately. There were no Facebook pages tracking Conor’s progress. The day we launched the website for Conor’s charity was very emotional for me. I feel like he is out there now in the big world now with his charity. He will never get to do the things that most 18-year-olds do. He won’t go inter-railing in the summer, he’ll never go bungee jumping off some bridge, but I feel that he’s part of the world, doing something good for other children and their families. We valued our time with Conor so much, we want to help researchers who will give families, even more time, more options, perhaps even a cure for their children when they get the same awful news that we did. I think he would approve of that.”




 “
“