We will work closely with the Conor Foley Neuroblastoma Cancer Research Foundation – a research charity led by the family who lost their child to neuroblastoma. An inspirational example of never giving up.
We will continue to dissect neuroblastoma biology using innovative platforms such as tumour-on-chip and 3D scaffold-based models in collaboration with our colleagues in the Tissue Engineering Research Group at RCSI and the Fraunhofer Project Centre at DCU.
This announcement is timely to celebrate Childhood Cancer Awareness Month in September.
Two talented and dedicated young scientists are joining our team. In 4 years time, we will have another pic of their graduation on the same stairs.
Every year, we celebrate Childhood Cancer Awareness Day Internationally. Pre-COVID times, it was straightforward to do a coffee morning, a bake sale, or as we did a Hot Chocholate morning.
To be honest with you, I had almost no presence of childhood cancer in my life until I joined Prof Stallings lab in 2011. When I said ‘almost’, I meant during my adulthood.
My Dad had a younger brother, both started their families at the same time. Our families used to spend a good time together, holidays, birthdays and weekends together. Both I and my cousin Igor were born almost within a year. I remember our play days together but at the level of feelings and stories told by my parents. In the pic, we were held by my nanna.
I do not have a pic where we were 3- or 4-years old. No pic was taken after Igor was diagnosed with blood cancer. He was 1-1.5-year-old. He travelled 800km to the best paediatric oncologists to receive the most progressive treatment back then. It extended his time with the family by four years. But he lost his battle…
How much can remember a 1-, 2-, 4- years old? My last memory – Igor was sleeping in a neat coffin. Adults were muttering. I remember, a tear slowly rolled down from Igor’s closed eyes. I naively asked my nanny why did the dead cousin cry??? He did not want to leave us, – said my nanny softly.
Back then parents were not much informed on the disease, treatments, odds and alternative options. Igor was suffering, no pain relief options were available… No palliative care… Remember my nanny’s words: “These doctors had no hearts. All this child needed was a sense of peace, quiet time with his parents away from the hospital wards”.
Many things have changed since then. Eight out of 10 children with blood cancer are responding to treatment well, they reach adulthood, may even have kids of their own. However, there are some types of childhood cancers that do not respond well and can return to being more aggressive. Cancer steals the child’s future. One of the thieves is neuroblastoma, a solid tumour of undeveloped nerves.
Childhood cancer research is essential to return happy days to kids and their families. Many childhood cancer research charities do their best to secure funds and support researchers like me. It is vital to have a continuous investment in research that helps to understand the weakness of childhood cancer and develop new drugs designed exclusively for kids.
Since I joined neuroblastoma research, I have been puzzled by the fact that half of the children with neuroblastoma have the disease spread at the time of diagnosis. It is still a puzzle whether cells spread and primary tumour growth happen simultaneously or more adventurous cancer cells escape the primary tumour location later.
At a cancer conference, I met Prof Ewald who studies this process in breast cancer. I was fascinated by the approach and started to look for opportunities to join his lab. To tell the truth, very few exist for mid-stage career scientists! One of them is the Fulbright program.
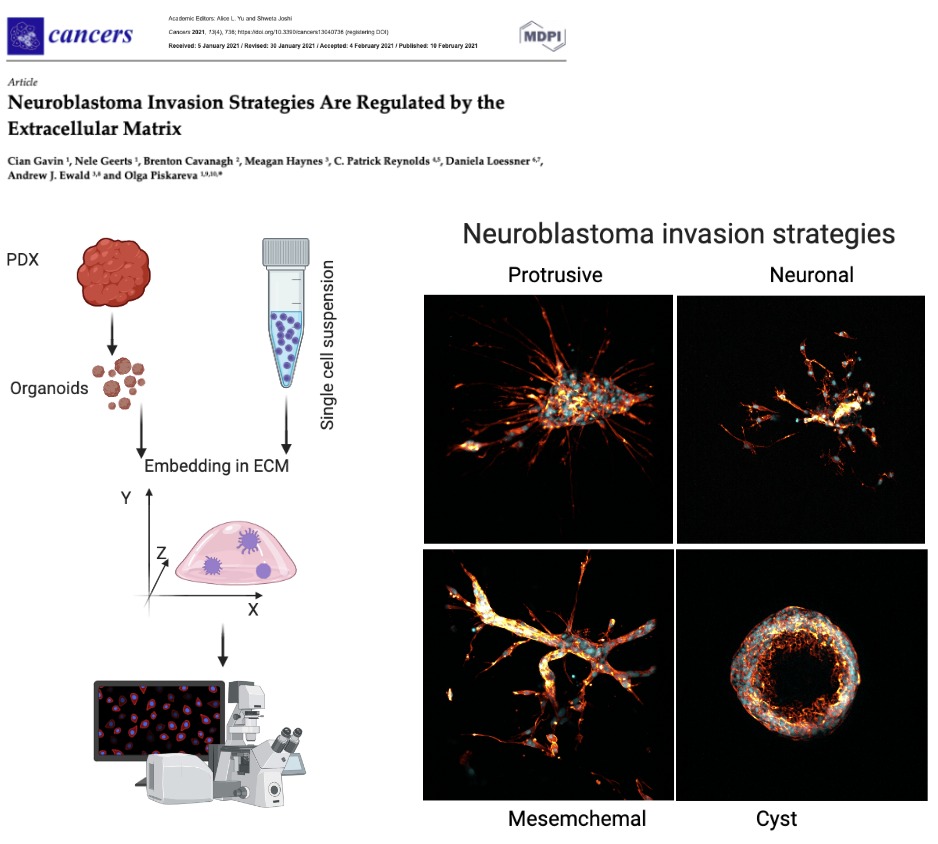
One day, I opened my email saying that I received a Fulbright-HRB Health Impact Scholar Award to travel to Johns Hopkins University and adapt their 3D models to learn how neuroblastoma spreads. It was a life-changing experience both personally and professionally. The amount of experimental data collected over 4 months of work did not fit a 1TB memory stick! Indeed, this short journey was just a start of a new research inquiry.
On my return home, the greatest task that remained was to make sense of every single experiment. Cian Gavin took over and spent almost a year systematising, characterising it, and placing it into a context. It was meticulous work with very little known about invasion strategies in neuroblastoma. Now, we are happy to share our findings published on Cancers.
Where do we go now? Well, our next step is to understand the cellular players behind neuroblastoma invasion and how we can target them to stop neuroblastoma spread. It won’t be a short and sweet journey, but we are ready for it!
This fantastic and rewarding work was supported by Fulbright Commission Ireland, National Children’s Research Centre, Health Research Board, Science Foundation Ireland, the National Institutes of Health/National Cancer Institute (Prof Ewald), Alex’s Lemonade Stand Foundation for the COG Childhood Cancer Repository (Prof Reynolds) and the National Institutes of Health/National Cancer Institute (Prof Reynolds).
Last month we set ourselves the “10 Laps 10km” challenge for Childhood Cancer Awareness.
Now we have closed the GoFundMe and counted the charity buckets. We are delighted to announce we raised a grand total of €1419! We are over the moon with this sum, as 2020 required a very different kind of fundraiser than previous years.
Our three chosen charities: Children’s Health Foundation Crumlin (formerly CMRF), the Conor Foley Neuroblastoma Cancer Research Foundation, and Neuroblastoma UK, will each receive just over €470.
We’d like to say big thank you to everyone who donated. It will make a huge difference for these charities, this year especially, paving the way to better treatment options for children with cancer in the future.
The new norm, new challenges, new excitement and new achievements! We all proud to say that we completed 10K Vhi Womens Mini marathon socially distanced. Our paces were so different that distancing came absolutely natural. We ran it individually but were a team mentally. Even the capricious Irish weather was our ally. The Sun was bright. The air was fresh and crispy.
This was an individual challenge #POWEROF10: just you and the trail. 10 laps around St Stephen’s Green park were to make the target 10K in aid of Childhood Cancer Awareness Month. The celebration of life, therapeutical advancements, the strength of little patients battling their cancer and their families, doctors and carers who are supporting them in their journey. The emphasis on the gaps in available treatments and diagnosis and the importance of research that needs funding.
Personally, my 10K were split into two parts. The first 4K were full of arguments with my body. Why didn’t I like to do laps? Could I complete 10K? Was I fit to do it? Keep going! No walking – better slow jogging. Did one lap make 1K? Should I do a longer lap instead? And so on and so forth. Then, the second part kicked in. My body stopped arguing and began to enjoy it. I noticed beautiful Autumn colours on the trees, people walking around with a cup of coffee or chatting away, saw my team members overtaking me, and our volunteers counting our laps. People on the street and in the park were cheering us up. What a wonderful and fulfilling day!
As Catherine says: “The 10 Laps 10km challenge was tough! Like many people, I took up running casually during the lockdown, however, I never did more than a couple of kilometres at once, so I was absolutely not prepared for running 10. But the cheers from our socially distanced spectators and all the online support we received meant I got through it. Also knowing what a positive impact this challenge could have for the future of childhood cancer treatment provided plenty of motivation to finish the race 💛🎗”
10K by 6 team members socially distanced. #POWEROF10. Go Gold! Let’s reach 1.5k in donations!
Our Go Fund Me page is still open until this Sunday (October 11th midnight) if you wish to support us.
This summer I worked under Dr Piskareva supervision in the remote research program. My original plans for a lab experience were put down by COVID. My ultimate goal was to write the review article on the potential uses of retinoic acid in neuroblastoma research.
Nadiya Bayeva
Before starting the project, I didn’t have any specific expectations. While I always had fun picking the primary articles apart and summarising the gathered data during my undergrad and med school, I didn’t believe that this experience would be the special one. And I kept thinking so as I was collecting the information from the numerous data on cell cultures. And as I was looking at the mice models studies. And clinical trials.
Then I started to write my introduction, and so researched the information on the neuroblastoma prognosis, contemporary treatment protocol and outcomes. And suddenly I saw my project in the new light. I was used to regarding the clinical trials outcomes as simple statistics, but this time no desensitization could shield me. Yes, 60% of the patients in the high-risk group die in 5 years after diagnosis, and yes, 90% of those patients are children less than 5 years old. And there is nothing that we could currently do to save those children.
On the other hand, this realisation brought meaning to my work. This time, I was not doing a PubMed search to get a good mark or CV reference. Instead, I was looking for the possible treatment of the disease. My review on the current knowledge about retinoic acid will let the other primary researchers target the most promising drug for future experiments and, eventually, create a novel and effective therapy to help those children.
And isn’t it what we are all striving for in medical research?
Today marks the start of Childhood Cancer Awareness Month.
Three girls fountain in Mainz Germany
I like this photo of a lovely fountain capturing 3 girls under umbrellas (Drei-Mädchen-Brunnen) in Ballplatz Mainz. It is about a happy childhood; every child deserves a happy childhood. So, I select it again to support #ChildhoodCancerAwarnessMonth.
Childhood cancer is an umbrella term for many other types of this disease. This month is a big channel to support and learn more about kids with cancer, their loving families, the doctors and caregivers who looking after them and treating them, the young survivors of cancer and those kids and teens who lost their battle, and the scientists who working hard to find a way to stop childhood cancer.
When it comes to a disease, we have to acknowledge that children are not little adults. They are constantly developing. So their diseases have a different way to progress and respond to treatment. This is very true for childhood cancers. For example, children diagnosed with neuroblastoma before a 1.5 years old mark will do better than older children.
Every 100th cancer patient is a child. Cancer is the 2nd most common cause of death among children after accidents. The most common types of childhood cancer are:
Leukaemia and lymphoma (blood cancers)
Brain and other central nervous system tumours
Muscle cancer (rhabdomyosarcoma)
Kidney cancer (Wilms tumour)
Neuroblastoma (tumour of the non-central nervous system)
Bone cancer (osteosarcoma)
Testicular and ovarian tumours (gonadal germ cell tumours)
Here, we are – the Irish neuroblastoma research team landed at the 5th Neuroblastoma Research Symposium in Cambridge. Four poster presentations by four enthusiastic scientists. The two days crash course in neuroblastoma – vibrant, intense, informative.
I had one of the most enjoyable poster sessions in the last few years! A genuine interest in our 3D in vitro cancer models by both academics and Industry. Hope, to keep the ball rolling and strengthen these new links.
The Symposium programme was an excellent balance of the new transnational outcomes with hardcore developmental cellular programmes. From ‘How neuronal precursors select their fate and how they can escape the developmental constraints? How this knowledge can help to advance our understanding of neuroblastoma aetiology?’ to ‘New drugs that demonstrated great potency in pre-clinical studies’ via ‘how we can work together more efficiently to progress quicker’
Indeed, the success of the research meeting became possible thanks to the strategic vision and leadership of organisers!
13:00 – 13:10 Introduction – Neuroblastoma UK & CRUK Cambridge Centre
Session 1: Neuroblastoma biology & prognosis
Cancer Research UK Cambridge Centre Neuro-oncology Programme Session
Chair: Kate Wheeler (Oxford Children’s Hospital)
13:10 – 13:40 Sandra Ackermann (Cologne): The genetic basis of favourable outcome and fatal tumour progression in neuroblastoma
13:40 – 14:10 Rogier Versteeg (Amsterdam): The dark side of neuroblastoma
14:10 – 14:40 Katleen de Preter (Ghent): Improved diagnosis and risk stratification of paediatric cancers using liquid biopsies
14:40 – 14:55 Sue Burchill (Leeds): Self-renewing neuroblastoma cells isolated from bone marrow aspirates of children with stage M disease share a mesenchymal expression signature: an NCRI CCL CSG Neuroblastoma Group Study
14:55 – 15:15 Combined discussion
15:15 – 15:45 Tea with Posters
Session 2: Targeted & combination therapy I
Cancer Research UK Cambridge Centre Neuro-oncology Programme Session
Chair: Marie Arsenian Henriksson (Karolinska)
15:45 – 16:15 Frank Westermann (Heidelberg): Novel metabolic dependencies of MYCN-driven neuroblastoma
16:15 – 16:45 Gerard Evan (Cambridge): Is Myc really master of the universe?
16:45 – 17:00 Melinda Halasz (University College Dublin): Anti-Cancer Effects of Diphenyleneiodonium Chloride (DPI) In MYCN-Amplified Neuroblastoma
17:00 – 17:15 Evon Poon (ICR, Sutton): Pharmacological blockade of high-risk MYCN driven neuroblastoma using an orally-bioavailable CDK2/9 inhibitor
17:15 – 17:35 Combined discussion
Downing College – Main Hall.jpg
17:35 – 19:15 Poster viewing & Drinks
19:30 Symposium Dinner at Downing College (map for dinner)
FRIDAY 12TH APRIL 08:30 – 08:50 Coffee & pastries
Session 3: Neural crest & differentiation therapy I
Chair: Margareta Wilhelm (Karolinska)
08:50 – 09:20 Igor Adameyko (Karolinska): Normal development of sympathoadrenal system resolved with lineage tracing and single cell transcriptomics
09:20 – 09:50 Quenten Schwarz (Adelaide): Guiding sympathoadrenal neural crest cells to the adrenal primordia
09:50 – 10:05 Claudia Linker (King’s College London): Notch coordinates cell cycle progression and migratory behaviour leading to collective cell migration
10:05 – 10:20 Combined discussion
10:20 – 10:50 Coffee with Posters
Session 4: Neural crest & differentiation therapy II
Chair: Gareth Evans (York)
10:50 – 11:20 Karen Liu (King’s College London): ALK and GSK3 – shared features of neuroblastoma and neural crest
11:20 – 11:35 Anestis Tsakiridis (Sheffield): Efficient generation of trunk neural crest and sympathetic neurons from human pluripotent stem cells via a neuromesodermal progenitor intermediate
11:35 – 12:05 Anna Philpott (Cambridge): Using developmental mechanisms to drive differentiation of neuroblastoma
12:05 – 12:20 Combined discussion
12:20 – 13:20 Lunch with Posters
Session 5: Targeted & combination therapy II
Chair: Bengt Hallberg (Gothenburg)
Cancer Research UK Cambridge Centre Paediatrics Programme Lecture:
13:20 – 13:50 Sharon Diskin (Philadelphia): A multi-omic surfaceome study identifies DLK1 as a candidate oncoprotein and immunotherapeutic target in neuroblastoma
13:50 – 14:05 Donne Nile (Glasgow): Manipulation of cancer cell metabolism for neuroblastoma combination therapy with targeted radiotherapy
14:05 – 14:35 Suzanne Turner (Cambridge): CRISPR-dCas9 screens to identify resistance mechanisms to ALK in neuroblastoma
14:35 – 14:50 Combined discussion
14:50 – 15:20 Tea with Posters
15:20 – 15:30 Poster prizes
Session 6: Targeted & combination therapy III
Chair: John Lunec (Newcastle)
15:30 – 16:00 Per Kogner (Karolinska): The PPM1D encoded WIP1 phosphatase is an oncogene significant for cancer development and tumour progression and a druggable therapy target in neuroblastoma and medulloblastoma. A hint as to how aggressive childhood cancer manages with wild-type p53
16:00 – 16:15 Deb Tweddle (Newcastle): Preclinical assessment of MDM2/p53, ALK and MEK inhibitor combinations in neuroblastoma
16:15 – 16:30 Sally George (ICR, Sutton): A CRISPR-Cas9 genomic editing and compound screening approach identifies therapeutic vulnerabilities in the DNA damage response for the treatment of ATRX mutant neuroblastoma
16:30 – 16:45 Miriam Rosenberg (Jerusalem): Expression- and immune-profiling of neuroblastoma-associated Opsoclonus Myoclonus Ataxia Syndrome (OMAS) to identify features of auto- and tumour-immunity
Across countries and continents, we are celebrating International Childhood Cancer Day (ICCD).We do it to raise awareness tto raise awareness of childhood cancer, its consequences for children and their parents and make it as a priority for Governments and research.
My team research is focused on neuroblastoma biology. This is a solid tumour of undeveloped nerves. Some forms of neuroblastoma spread quickly and become very aggressive and challenging to treat. We are searching for the weaknesses that can be targeted with drugs.
A guessing game was a part of the event. Everyone had a chance to guess how many marshmallows fitted in the cell culture flask T75. The guesses ranged from as low as 95 to as high as 500. Fortunately, one of the participants gave an absolutely correct answer. Micheal Flood put on 173 and won. Her fantastic ability to guess is incredible! Congratulations!!! Well done to all!
We raised 698.91 Euros for childhood cancer research! We thank everyone who came along and supported the Hot Chocolate Morning & the International Childhood Cancer Day 2019!
Many special thanks go to Amorino for delicious Italian hot chocolate & tasty bites contributors!
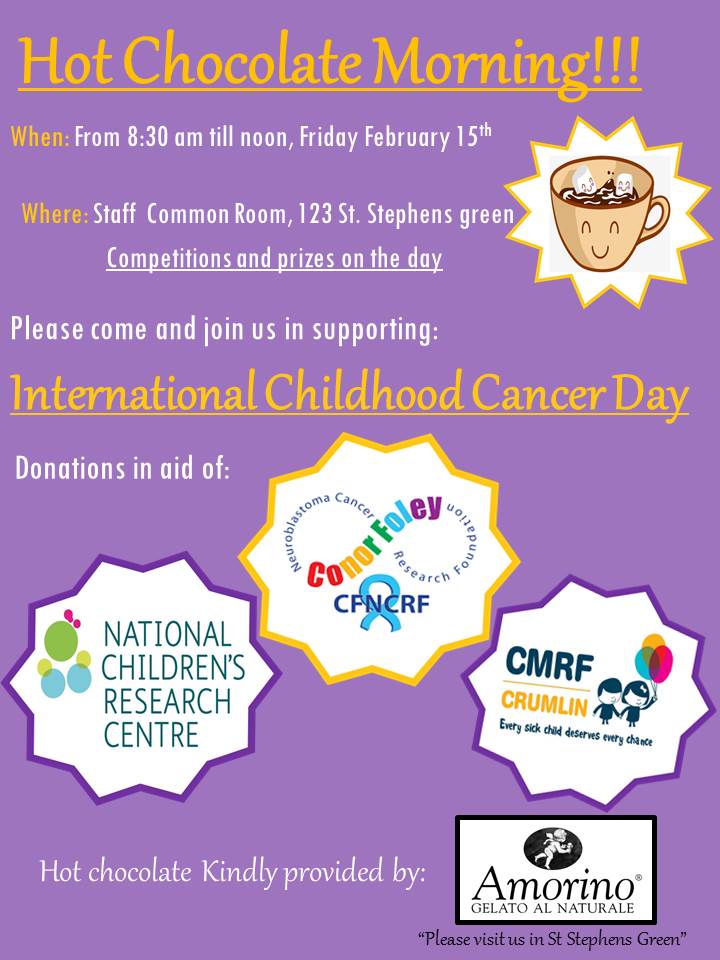
International Childhood Cancer Day (ICCD) was founded in 2002 by Childhood Cancer International (CCI). Each year on February 15th we unite together to recognise childhood cancer as a national and global child health priority & to raise support, funding and awareness of this devastating desiease.
This year we team up with Amorino to run Hot Chocolate Morning. Please come along! All proceeds go to CMRF/NCRC and CFNCRF.