

Another year, another Research Summer School students. We are hosting 4 students (Jessica, Dawn, Dola, and Jeff) this year. Some of them will be medical doctors, another will do research after the graduation. For them, the 8-weeks lab placement is a window into the reality of the everyday science. How cancer cells look? How do they grow? Where do we store them? How do we know that we have identified a new drug or a new target to study further? Do researchers have a sense of humour? Do they like donuts?
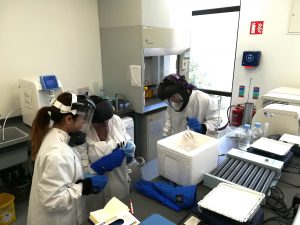
We have already said Good Bye to Jessica. Dola and Dawn’s projects are coming to an end this week, while Jeff is staying till the end of August.


 “
“

