Anti-cancer vaccines teach the body’s immune system to identify and attack tumour cells. They are a type of immunotherapy and can be used to treat cancer or prevent tumour recurrence. Therefore, they are typically used in patients that have already received other treatments such as surgery, chemotherapy or radiotherapy.
Although anti-cancer vaccines have been gaining more attention over the years, few are being developed for paediatric tumours. From 594 clinical trials in neuroblastoma at clinicaltrials.gov, only 12 active trials are evaluating vaccines. Furthermore, these vaccines are still considered investigational products. They do not have the approval for use granted by health authorities. Therefore, these drugs are available for patients that enter into clinical trials.
An example of these vaccines is the bivalent vaccine for high-risk neuroblastoma developed in the Memorial Sloan Kettering Cancer Center in the US, collaborating with the biopharmaceutical company Y-mAbs Therapeutics. This vaccine is called bivalent because it has two proteins specifically present on the surface of neuroblastoma cells.
The rationale behind the treatment using this vaccine is that the body will be stimulated to produce antibodies against these two proteins. These antibodies will recognise and attach to neuroblastoma cancer cells, thus signalling to the immune system that these cells need to be eliminated. A phase II trial evaluates vaccine efficacy in 374 patients who received seven subcutaneous injections of the vaccine in combination with an oral intake of an adjuvant, called β-glucan, that boosts the immune system1. The adjuvant intake started either on the first vaccine injection or on the third injection every two weeks until the end of the vaccine schedule. The study aims to analyse the anti-tumour effect of the vaccine and the immune response generated by the vaccine plus β-glucan therapy. The study is estimated to be completed by 2023. The trials active for neuroblastoma vaccines are phase I or II. After these phases, there are still phases III and IV to complete the evaluation and continue monitoring these therapies. Therefore, in a few more years, we will know if neuroblastoma vaccines will be successful or not.
Written by Luiza Erthal
Reference
1. Memorial Sloan Kettering Cancer Center. Phase I/II Trial of a Bivalent Vaccine With Escalating Doses of the Immunological Adjuvant OPT-821, in Combination With Oral β-glucan for High-Risk Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT00911560 (2021).
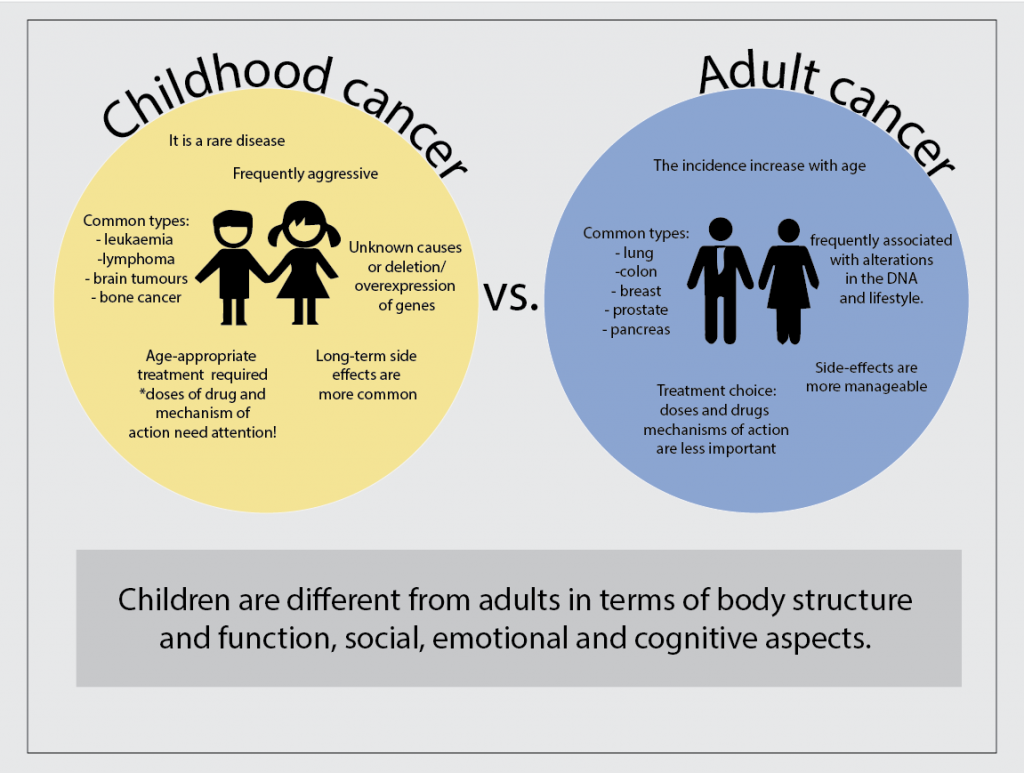
Looking carefully we can easily see that children are very different from adults. They have different needs, desires, likes and dislikes. Not surprisingly, the children body is also very different in their functioning and response to medical needs. Therefore, cancer in children has many different characteristics when compared to cancer in adults. Childhood cancer is different in terms of the most common types, the causes, the treatment and the course of the disease.
Firstly, childhood cancer is rare and this sometimes impairs an early diagnosis. Therefore more aggressive diseases tend to be present at the time of diagnosis. Nevertheless, there are specific types of cancer that are more common in children, which helps in the diagnosis. They are cancers affecting the blood and lymph nodes (leukaemia and lymphoma), the brain (astrocytoma), the liver and the bones (osteosarcoma). These types of cancer are less common in adults.
Another important difference between adult and childhood cancer is the leading cause of the disease. Most of the time the cause of childhood cancer is unknown, although genetic contributions related to overexpression or deletion of genes can be determined. On the other hand, adult cancers are frequently associated with alterations in the DNA (mutations) as well as lifestyle.
The treatment plays an important role in the differences between adult and childhood cancers. Usually, similar treatments are used for both adults and children, including chemotherapy, radiotherapy, surgery, transplants and immune therapy, according to the type of cancer and its stage. However, the doses and types of drugs may differ between them. The differences in the treatment go beyond the doses and encompass the mechanisms of action and possible long term toxicities of drugs. For example, the use of drugs that damage DNA can be prohibitive in children due to the increased risk of secondary cancers in the future.
In conclusion, specific types of cancer are more common in children and the cause of this disease is frequently unknown. Fortunately, children have great possibilities to survive cancers but the treatment needs to be carefully chosen and its long-term effect on the body have to be monitored for their whole life.
Written by Luiza Erthal
References
Kattner, P. et al. Compare and contrast: pediatric cancer versus adult malignancies. CancerMetastasis Rev. 38, 673–682 (2019).
Neuroblastoma relapse is one of the greatest challenges to complete cure for children with high-risk disease. At least 40% of high-risk neuroblastoma patients will experience cancer relapse 4 years after intense treatment, which includes a combination of chemotherapy, surgery, irradiation and the self-transplantation of stem cells (consolidation therapy).
To overcome this problem improved maintenance therapy is needed. These are therapies administered to patients after the end of the initial treatment to prevent tumour relapse. Frequently, maintenance therapy for neuroblastoma includes immunotherapies such as antibodies against GD-2 and cytokines and 13-cis-retinoic acid. Although these therapies have some positive effects, the rate of relapse is still high. Therefore, other options to prevent relapse are needed.
Recently, a phase II clinical trial evaluated the effect of Difluoromethylornithine (DFMO) on event-free survival (EFS) and overall survival (OS) of high-risk neuroblastoma patients1. Event-free survival means the length of time that the patient remains free of cancer after the end of treatment, while overall survival means the length of time that the patient is alive after the diagnosis or the start of treatment. The measurement of event-free survival and overall survival provides a good indication of the treatment effect.
In this clinical trial report the therapy efficacy on 81 patients that received immunotherapy treatment with dinutuximab and started DFMO maintenance therapy at least 120 days after completion of treatment were compared to the efficacy (based on medical records) from a group of 76 patients that got the same treatment but without the maintenance with DFMO.
DFMO inhibit the ornithine decarboxylase pathway, which is related to cell growth and decreased cell death, thus preventing cells to become cancerous and tumour progression. The results demonstrated that maintenance therapy with DFMO provided 85% of 5-year event-free survival compared to 65% for no-DFMO maintenance therapy, and 95% 5-year OS compared to 81% no-DFMO therapy2.
In conclusion, this study results suggest a benefit provided by the DFMO therapy in preventing neuroblastoma relapse. The researchers suggest that early therapy with DFMO may further improve these results. Therefore, more clinical trials evaluating this possibility are being conducted3,4.
Written by Luiza Erthal
References
1. SaulnierSholler, G. A Phase II Preventative Trial of DFMO (Eflornithine HCl) as a Single Agent in Patients With High Risk Neuroblastoma in Remission. https://clinicaltrials.gov/ct2/show/NCT02395666 (2020).
2. Lewis, E. C. et al. A subset analysis of a phase II trial evaluating the use of DFMO as maintenance therapy for high‐risk neuroblastoma. Int. J. Cancer 147, 3152–3159 (2020).
3. SaulnierSholler, G. Phase II Trial of Eflornithine (DFMO) and Etoposide for Relapsed/Refractory Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT04301843 (2021).
4. SaulnierSholler, G. NMTT- Neuroblastoma Maintenance Therapy Trial Using Difluoromethylornithine (DFMO). https://clinicaltrials.gov/ct2/show/NCT02679144 (2021).
Immunotherapies are treatments that stimulate the patient’s immune system to help it to fight cancer. This type of treatment is gaining more attention in neuroblastoma due to the possibility to combine it with other therapies, potentially, generating fewer side effects.
Clinical trials are research protocols performed in patients to evaluate whether a new treatment is safe and effective. This type of research can also compare standard treatments with new treatment options as well as investigate new combinations of drugs. Clinical trials occur in phases comprising phase I (safety), phase 2 (safety and efficacy), phase 3 (safety, efficacy and comparison with standard treatments for the specific disease).
According to a search performed on November 14th, 2021, there are 594 clinical trials for neuroblastoma at clinicaltrials.gov, a clinical trial database from the United States (US). From these, 173 are recruiting or active trials and 15 are related to immunotherapies. Generally, these are initial trials evaluating treatment combinations using chemotherapy, cell transplants and immunotherapy, including antibodies and vaccines.
Trials for antibodies
The most explored target for immunotherapy in neuroblastoma is the GD2, a molecule present in the surface of neuroblastoma cells that can be used to combat the tumour. Indeed, antibodies that bind to GD2 called dinutuximab and naxitamab are approved for use in the US to treat neuroblastoma1,2.
A clinical trial in the US and Canada is recruiting patients to evaluate the combination of dinutuximab with another antibody called Magrolimab in patients with neuroblastoma that do not respond to or come back after treatment3. This is an initial trial (Phase 1), which aims to determine the best doses and side effects of this combination.
Racotumomab, an antibody that binds to N-glycolyl GM3, a molecule that is highly expressed in the surface of neuroblastoma cells, is being evaluated in high-risk neuroblastoma5. The study aims to determine the immune response generated by the drug and the related toxicity.
Trials for vaccines
A trial from Dana-Farber Cancer Institute is recruiting patients to study the GVAX Vaccine and its combination with the antibodies, nivolumab and ipilimumab, that stimulates T-cells to attack the cancer 6. The vaccine is produced with neuroblastoma cells from the patient. The study will evaluate the dose and safety of the combination treatment.
Another trial is evaluating the use of a modified neuroblastoma cell vaccine in combination with low doses of chemotherapy (Cytoxan/Cyclophosphamide)7. A vaccination scheme comprising 8 doses of vaccine and cycles of oral chemotherapy is planned and patients will be closely monitored through the vaccination period to evaluate side effects and disease status. This study is ongoing and will follow the patients for 15 years after completing the vaccination scheme.
Trials for cell therapy
A trial evaluating the use of modified T-cells (CART-T-cell) to recognise GD2- neuroblastoma cells in combination with chemotherapies (cyclophosphamide and fludarabine) and an antibody (Pembrolizumab) is ongoing8. The combination is based on previous studies that have demonstrated the longer time presence of CAR T-cell in the blood of patients after intravenous infusion of chemotherapy. Moreover, the antibody will help to stimulate the patient immune system. The trial aims to determine the highest dose possible for the combination treatment generating fewer side effects.
Another Phase I immunotherapy trial for neuroblastoma aims to compare the treatment with dinutuximab and lenalidomide (drugs that support the immune system) and Natural Killer (NK) cells from the patient9. The NK cells can kill cancer cells while the two immunotherapeutic drugs activate the NK cells. This study will determine the safest dose of cells to be used in combination with the drugs.
Conclusion
Considering some of the clinical trials in progress that uses immunotherapy to treat neuroblastoma, we can conclude that this therapy modality holds great promise to advance and potentially serve as a new treatment option to improve neuroblastoma patients’ survival and quality of life.
Written by Luiza Erthal
References
1. Drugs Approved for Neuroblastoma – National Cancer Institute. https://www.cancer.gov/about-cancer/treatment/drugs/neuroblastoma (2011).
2. Memorial Sloan Kettering Cancer Center. Expanded Access Use of Naxitamab/GM-CSF Immunotherapy for Consolidation of Complete Remission or Relapsed/Refractory High-Risk Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT04501757 (2021).
3. National Cancer Institute (NCI). Phase 1 Trial of Hu5F9-G4 (Magrolimab) Combined With Dinutuximab in Children and Young Adults With Relapsed and Refractory Neuroblastoma or Relapsed Osteosarcoma. https://clinicaltrials.gov/ct2/show/NCT04751383 (2021).
4. Memorial Sloan Kettering Cancer Center. Hu3F8/GM-CSF Immunotherapy Plus Isotretinoin for Consolidation of First Remission of Patients With High-Risk Neuroblastoma: A Phase II Study. https://clinicaltrials.gov/ct2/show/NCT03033303 (2020).
5. Laboratorio Elea Phoenix S.A. Open-label, Multicenter, Phase II Immunotherapy Study With Racotumomab in Patients With High-risk Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT02998983 (2021).
6. Collins, N. B. A Phase 1 Study of Combination Nivolumab and Ipilimumab With Irradiated GM-CSF Secreting Autologous Neuroblastoma Cell Vaccine (GVAX) for Relapsed or Refractory Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT04239040 (2021).
7. Heczey, A. A Phase I/II Study Using Allogeneic Tumor Cell Vaccination With Oral Metronomic Cytoxan in Patients With High-Risk Neuroblastoma (ATOMIC). https://clinicaltrials.gov/ct2/show/study/NCT01192555 (2021).
8. Heczey, A. Autologous Activated T-Cells Transduced With A 3rd Generation GD-2 Chimeric Antigen Receptor And iCaspase9 Safety Switch Administered To Patients With Relapsed Or Refractory Neuroblastoma (GRAIN). https://clinicaltrials.gov/ct2/show/NCT01822652 (2021).
9. New Approaches to Neuroblastoma Therapy Consortium. A Phase I Dose Escalation Study of Autologous Expanded Natural Killer (NK) Cells for Immunotherapy of Relapsed Refractory Neuroblastoma With Dinutuximab +/- Lenalidomide. https://clinicaltrials.gov/ct2/show/NCT02573896 (2021).
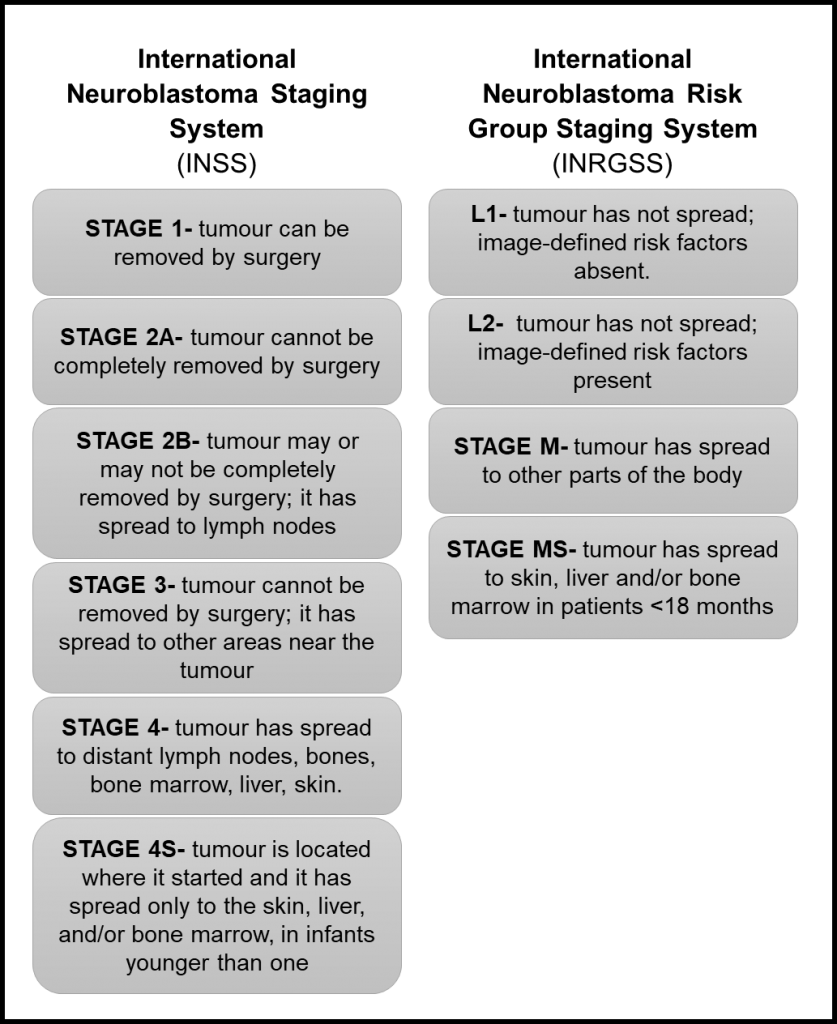
The determination of the tumour stage is an important step after a neuroblastoma diagnosis. The stage of neuroblastoma is determined depending on tumour location and if it has spread to other parts of the body. This will guide risk group assignment and treatment choice.
The first staging system for neuroblastoma, the International Neuroblastoma Staging System (INSS), was developed in 1986 and is based on the pathological evaluation of the tumour after a removal surgery. In 2005, The International Neuroblastoma Risk Group Staging System (INRGSS) started to be used. This system is based on tumour images before any surgery. Therefore, it is based on image-defined risk factors to determine the tumour stage (see table below). It also uses clinical, pathologic, and genetic markers to determine the risk groups, which can be low-risk, intermediate-risk, or high-risk.
Reference: Neuroblastoma – Childhood: Stages and Groups, Cancer.net.
Recently, the Children’s Oncology Group (COG), a clinical trial group dedicated to paediatric cancer research revised the classification system they use to determine tumour stage for enrolment in clinical trials1. Previously, they have been defining the tumour stage based on the INNS system. Now they proposed a revised classification that takes into account the INRGSS and chromosomal alterations.
Key clinical and biological factors used in the neuroblastoma risk classification include age at diagnosis, disease stage, tumour tissue appearance under a microscope (histology), the status of the gene MYCN that affects tumour growth, the amount of DNA in a tumour cell (called tumour cell ploidy), and alterations in the DNA.
They analyse the outcome of almost 5,000 patients to define risk groups based on the INRGSS, using alterations in the DNA of tumour cells as a biomarker and considering current therapy modalities. In general, they found that the correlation of stages between systems is not exact. However, the differences in survival were minimal when comparing staging systems, which corroborates the use of the revised version.
In general, the new version classifies L1 and L2 tumours as low risk, except for L1 tumours with alteration in the gene MYCN and that cannot be removed by surgery, which is high-risk. For L2 tumours, MYCN status and age can be used to evaluate prognosis. Stage M tumours can be classified as high risk or intermediate-risk depend on age, MYCN status and DNA alterations. In conclusion, low-risk groups have excellent outcomes with any or limited therapy, the intermediate-risk group have very good outcomes and high-risk groups have inferior outcomes despite therapy.
This new version of the COG classifier will provide a uniformization of patient risk classification for clinical trials, ultimately enabling the comparison between different trials.
Written by Luiza Erthal
Reference:
1. Irwin, M. S. et al. Revised Neuroblastoma Risk Classification System: A Report From the Children’s Oncology Group. J. Clin. Oncol. JCO.21.00278 (2021)
We are launching a new initiative #AskLuiza to help the public and patients know more about advances and current trends in neuroblastoma.
Luiza is a research writer at the Cancer Bioengineering Research Group. She holds a PhD in Biomedical Sciences from Trinity College Dublin. You will ask a question and Luiza will look for the answer in peer-reviewed research papers that the research community trust.
Finding suitable research models to study disease is a big challenge for researchers around the world. In cancer research, it is essential to work with models that can recapitulate tumour characteristics as much as possible. This is important to test chemotherapeutic drugs, understand tumour behaviour and have higher chances of translating the finds from the laboratory to clinical practice.
Multiple factors influence tumour behaviour and disease progression. The most important is the tumour microenvironment, which comprises different cells and molecules that surround the tumour and the extracellular matrix, a network of molecules that provides support to the cells in the body.
Most cell studies in a laboratory are based on 2D cell culture models in which the cells grow in a monolayer. Although this approach has a low cost and it is easy to use, it lacks the complexity observed in the clinical scenario. It is true that no model can recapitulate all the complexity found in the body. However, scientists were able to develop interesting approaches to study different tumour characteristics with relatively good approximation1.
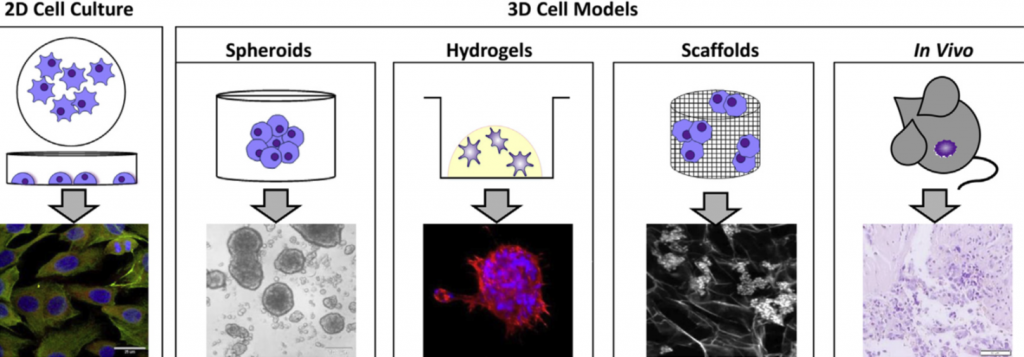
Specifically for neuroblastoma, the most common solid tumour that affects children, scientists developed 3D models in which neuroblastoma cells grow interacting with the surrounding environment and with each other in a vial. Examples of 3D models include cells grown in hydrogels or scaffolds and multicellular tumour spheroids (see image below). Spheroids are formed through the self-adhesion of tumour cells growing in the form of very small balls. They can be maintained in the laboratory on their own or supported by scaffold-based platforms (jelly-like or porous materials). Scaffolds essentially support the cell resembling the extracellular matrix and surrounding tissue in the body.
Credits for the image: 3D models to study neuroblastoma. Adapted from Nolan, J. C. et al. Preclinical models for neuroblastoma: Advances and challenges. Cancer Lett. 474, 53–62 (2020).
In the Cancer Bioengineering Research Group, we work with neuroblastoma models such as organoids, a more complex type of spheroid, to understand neuroblastoma migration and invasion2. Moreover, we recently shared with the research community a protocol at jove.com describing the development of a 3D neuroblastoma model using collagen-based scaffolds3.
Time-lapse video of neuroblastoma organoids’ growth. Accompanying experimental data published in Gavin et al., Cancers 2021. Source: the Cancer Bioengineering Research Group
These models have the potential to advance drug tests performed in the laboratory providing better clinical translation, ultimately contributing to improving the quality of life and survival of children diagnosed with neuroblastoma.
The work with 3D models at the Cancer Bioengineering Research Group is supported by the Irish Research Council, the Conor Foley Neuroblastoma Cancer Research Foundation, Neuroblastoma UK and National Children’s Research Centre.
Written by Luiza Erthal
References
1. Nolan, J. C. et al. Preclinical models for neuroblastoma: Advances and challenges. Cancer Lett.474, 53–62 (2020).
2. Gavin, C. et al. Neuroblastoma Invasion Strategies Are Regulated by the Extracellular Matrix. Cancers13, 736 (2021).
3. Gallagher, C., Murphy, C., O’Brien, F. J. & Piskareva, O. Three-dimensional In Vitro Biomimetic Model of Neuroblastoma using Collagen-based Scaffolds. J. Vis. Exp. 62627 (2021) doi:10.3791/62627.