It was February 2020, just before one of the biggest global pandemics struck, that I attended the IACR as a research assistant. It was my first official conference and it is safe to say ‘Imposter Syndrome’ was my main feeling going down to Galway on the train. Fast forward 2 years and my feelings travelling to IACR 2022 in Cork could not be more different. It is amazing what starting a PhD during a pandemic can do for your confidence and skills as a researcher – a sink or swim moment if there was ever one. My first IACR in Galway was one to remember surrounded by like-minded scientists, all brimming with new ideas and exciting discoveries. As such, I had high hopes for IACR 2022. And it did not disappoint.
Ellen King, PhD student at the IACR Meeting 2022
My PhD project focuses on the development of a vaccine to treat neuroblastoma so I was very excited to hear talks from some of the leading experts in vaccine research, both in industry and academia. I gained so much from hearing these experts discuss their research but also discussing other important topics like career progression and how to keep a work/life balance in research. It was refreshing to hear that as scientists we don’t have to (and shouldn’t) work ourselves to the bone 24/7 to be successful. As a young scientist planning to continue into academic research, this left a lasting impression on me. To top off what was already a hugely beneficial conference for me, my poster was shortlisted for a prize. I was shocked, delighted and excited all-in-one. Starting my PhD during a pandemic was not without challenges. Delays in deliveries, delays getting trained on equipment and multiple lockdowns led to what felt like (for me) quite a disjointed start. For my research to be shortlisted by experts was, to be honest, a relief. To know that my work stood out was extremely important to me and that all the hard work does pay off. When my name was called out at the Gala dinner as a Poster Prize Winner, all the doubts that I had (doubts that we all have as scientists) disappeared. I felt very proud and very grateful that my research was recognised at that level. There is no doubt that in-person conferences give a huge boost to young researchers, and I really look forward to presenting my work at the next IACR meeting.
At the beginning of my career, I worked for two years in a Ukrainian company organizing international industrial conferences. So I have insider knowledge of how the conference works, and that the determining factor for the success is the active communication between the participants. And at the RCSI research day and Cork IACR conference, this component was perfect. At both events, I presented my poster and had a chance to discuss the recent advances in neuroblastoma epigenetic drug research. During RCSI Research day, I was excited to learn about the accomplishments of other undergraduate studies and was thrilled to learn that my classmate is participating in research too. He had developed an online recourse to practice cardiac auscultation, which is extremely useful for my medical studies. But professionally, I enjoyed the cancer research posters and presentations at the IACR conference and was eager to meet the researchers working on medulloblastoma, a paediatric neural cell cancer, and the research team from UCD, the neighbours of our university who worked on breast cancer. It was the most valuable opportunity to take a glimpse into other research, become inspired by the most ingenious methods, and cultivate professional knowledge and personal connections – I am so lucky I have been at RCSI Research day and the IACR conference! I have greatly enjoyed my time, and I am looking forward to (hopefully) going to the next year’s conferences again.
Cancer Bioengineering Group thoroughly enjoyed getting back to in-person Research Day at RCSI after 2 years, we’re now very much looking forward to the IACR conference later this month! We will have 2 oral and 5 poster presentations at IACR 2022.
A typical day for me is difficult to describe because there are many facets to a PhD in the Cancer Bioengineering research group. Some days I spend in the lab sectioning, staining or looking at tumour samples under the microscope. Others I stay at home, read papers and try to figure out how they can help me to achieve my research goals. Some days I take part in the courses and workshops offered in the scope of a structural PhD. Then there are times when I sit here writing up for you guys what it is that I do those other days. The academic environment also provides lots of other opportunities to apply yourself and broaden your horizons or pursue what you enjoy. I, for example, have the chance to partake in weekly dissections for medical teaching which helps to keep my anatomical knowledge fresh and is an always welcome change of scenery (and smell) when I am stuck on other things. Furthermore, I get to see the other side of conferences and what is involved in their planning, because I am part of the local organising committee for the European Federation for Experimental Morphology Symposium 2022.
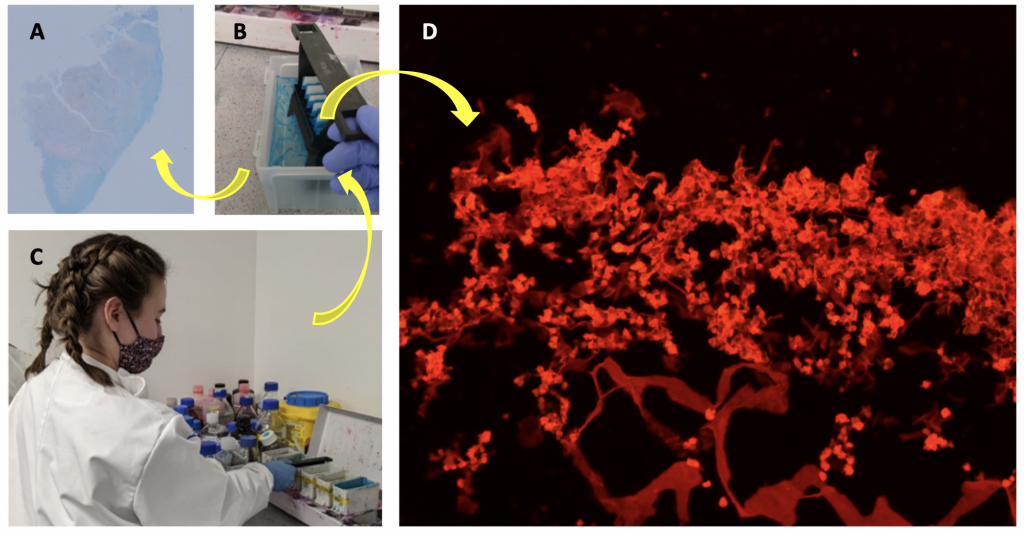
Figure 1 Working on neuroblastoma cancer the samples I am working with are quite unsurprisingly tumour cells. But these can be grown, for example, in mice (A) or on manmade scaffolds (D). I am moving a staining rack that holds the microscopy slides through staining containers filled with different solutions (C) to stain the slides. After the slides are stained the excess stain is removed by washing in distilled water (B). The resulting images depend on the type of stain. Stains like Alcian Blue can only be viewed with brightfield microscopy (A). But Picrosirius red can also be viewed under polarised light or as seen here (D) with fluorescent microscopy.
Currently, not yet half a year into my PhD, a lot of my time is spent planning. That’s planning which methods to use, which products to order and which experiments, and analyses would result in the most coherent and rounded off story being told by the summation of my research. I also spend a lot of time optimising the methods I will use to assure reproducibility and avoid issues during the analysis later on. For example, the whole tumour sample stained with Alcian blue you can see in Figure 1A clearly shows discernible blue and red regions. However, I have spent about 2 months now trying to get to a point of producing this same outcome reliably rather than having samples show up entirely blue or very only faintly stained. Picrosirius red, the solution I used to stain the sample in Figure 1D stains collagen. But there are many different stains for collagen. After researching most if not all of them I chose this one because it can be viewed with different types of microscopies providing slightly different information. Another step of planning includes how many pictures of which magnification will be required, one image of a whole section for orientation such as in Figure 1A and then more zoomed-in images to investigate the structure of collagen such as in Figure 1D.
Between course work and planning and optimising different aspects of my project, my PhD provides me with plenty of opportunities to focus on something else whenever I get stuck to later return with a fresh set of eyes.
Written by Ronja Struck, a 1st Yr PhD student funded by the IRC-CFNCRF
It is time for a full group presentation here at the blog! Throughout the month we shared about our group members and their research focus on Twitter. Now, we would like to share more about the group here and invite you to keep following us on social media.
The Cancer BioEngineering Group is a research group led by Dr Olga Piskareva at the Royal College of Surgeons in Ireland. The group has 6 PhD students developing research projects around neuroblastoma biology.
Our projects address topics related to neuroblastoma microenvironment, cell interactions, tumour resistance and the development of new therapies. To do that we use 3D in vitro models, identify immunotherapeutic targets and evaluate extracellular vesicles.
We are a dynamic group proud to be engaged in research, science communication and patient involvement. We do that through different initiatives.
We promote neuroblastoma awareness through different activities. For instance, last September at the Childhood Cancer Awareness month we promoted a hiking challenge to raise money and increase awareness of neuroblastoma. We hiked for 30km at Wicklow mountains in a day and raised over € 2,000 for neuroblastoma research charities.
We are also present in social media, creating content in the form of blog posts and tweets to share the science we are doing.
We are always happy to answer questions and interact with the public. Follow us on our social media channels and read our blog to know more about us and our research.
Thanks for reading and we go ahead with neuroblastoma research!
Understanding how tumour cells interact with the other cells in the body is crucial for an effective treatment. Moreover, it can help to identify patterns that are exclusive of tumour cells to be a target in treatment.
The interactions of tumour cells with the surrounding tissue, the microenvironment, affects chemotherapy sensitivity, immune cells recognition and expression of molecules on the cell surface, to only cite a few interferences.
This is particularly crucial in metastatic cells, which are cells that have spread to other parts of the body coming from the primary tumour location. Specifically, for neuroblastoma half of patients with high-risk disease present a metastatic tumour at the diagnosis. In addition, one of the organs that are mostly populated by metastatic neuroblastoma cells is the bone marrow.
A review paper recently published address some important aspects about the interactions between neuroblastoma cells, bone and bone marrow resident cells1. This review argues in favour of understanding these interactions to search for new targets for therapy.
However, neuroblastoma cells proved to be difficult to characterise due to dynamic changes induced by external stimuli. Therefore, neuroblastoma cells change upon exposure to the bone marrow microenvironment.
The authors present some studies showing that neuroblastoma cells infiltrating the bone marrow express receptors for small proteins called chemokines that induce cell adhesion in the bone marrow. On the contrary, the cells did not present on their surface molecules that stimulate the immune system recognition. Therefore, they are naturally invisible to the action of this system.
Moreover, it has been shown that metastatic tumour cells release extracellular vesicles expressing GD2. These vesicles have an important role in cell-cell communication and the GD2 is a marker exclusive of neuroblastoma cells. Thus, it facilitates the identification of metastatic cells.
These alterations on neuroblastoma cells surface after they interact with bone marrow cells may facilitate the invasion and spread of the tumour. Thus, looking closely to that may help to develop more effective treatments for neuroblastoma.
At the Cancer Bioengineering Research Group, many of our projects are related to tumour resistance, cell interaction and the tumour microenvironment. These three aspects are very important to understand neuroblastoma at the tissue level. We study them and expand this research to applied projects aiming at the development of new therapeutic modalities.
For instance, we are currently evaluating the effect of extracellular vesicles from different neuroblastoma cell lines in the induction of proliferation and increased viability. Moreover, we are studying the interaction of neuroblastoma cells with immune cells such as macrophages. Finally, we are also identifying targets to develop an anti-tumour nucleic acid-based vaccine against neuroblastoma.
We go from basic to applied research interconnecting the findings and expanding the understanding of neuroblastoma biology. Ultimately, we aim to improve treatment and quality of life for patients.
Written by Luiza Erthal
References
1. Brignole, C. et al. Bone Marrow Environment in Metastatic Neuroblastoma. Cancers13, 2467 (2021).
Anti-cancer vaccines teach the body’s immune system to identify and attack tumour cells. They are a type of immunotherapy and can be used to treat cancer or prevent tumour recurrence. Therefore, they are typically used in patients that have already received other treatments such as surgery, chemotherapy or radiotherapy.
Although anti-cancer vaccines have been gaining more attention over the years, few are being developed for paediatric tumours. From 594 clinical trials in neuroblastoma at clinicaltrials.gov, only 12 active trials are evaluating vaccines. Furthermore, these vaccines are still considered investigational products. They do not have the approval for use granted by health authorities. Therefore, these drugs are available for patients that enter into clinical trials.
An example of these vaccines is the bivalent vaccine for high-risk neuroblastoma developed in the Memorial Sloan Kettering Cancer Center in the US, collaborating with the biopharmaceutical company Y-mAbs Therapeutics. This vaccine is called bivalent because it has two proteins specifically present on the surface of neuroblastoma cells.
The rationale behind the treatment using this vaccine is that the body will be stimulated to produce antibodies against these two proteins. These antibodies will recognise and attach to neuroblastoma cancer cells, thus signalling to the immune system that these cells need to be eliminated. A phase II trial evaluates vaccine efficacy in 374 patients who received seven subcutaneous injections of the vaccine in combination with an oral intake of an adjuvant, called β-glucan, that boosts the immune system1. The adjuvant intake started either on the first vaccine injection or on the third injection every two weeks until the end of the vaccine schedule. The study aims to analyse the anti-tumour effect of the vaccine and the immune response generated by the vaccine plus β-glucan therapy. The study is estimated to be completed by 2023. The trials active for neuroblastoma vaccines are phase I or II. After these phases, there are still phases III and IV to complete the evaluation and continue monitoring these therapies. Therefore, in a few more years, we will know if neuroblastoma vaccines will be successful or not.
Written by Luiza Erthal
Reference
1. Memorial Sloan Kettering Cancer Center. Phase I/II Trial of a Bivalent Vaccine With Escalating Doses of the Immunological Adjuvant OPT-821, in Combination With Oral β-glucan for High-Risk Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT00911560 (2021).
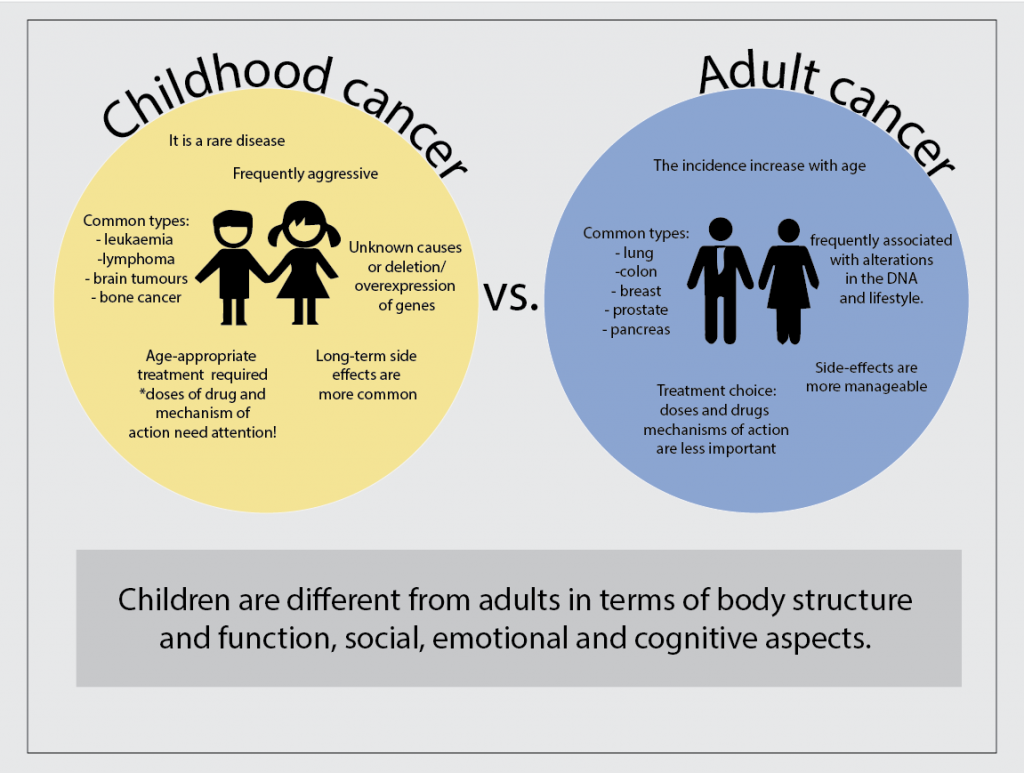
Looking carefully we can easily see that children are very different from adults. They have different needs, desires, likes and dislikes. Not surprisingly, the children body is also very different in their functioning and response to medical needs. Therefore, cancer in children has many different characteristics when compared to cancer in adults. Childhood cancer is different in terms of the most common types, the causes, the treatment and the course of the disease.
Firstly, childhood cancer is rare and this sometimes impairs an early diagnosis. Therefore more aggressive diseases tend to be present at the time of diagnosis. Nevertheless, there are specific types of cancer that are more common in children, which helps in the diagnosis. They are cancers affecting the blood and lymph nodes (leukaemia and lymphoma), the brain (astrocytoma), the liver and the bones (osteosarcoma). These types of cancer are less common in adults.
Another important difference between adult and childhood cancer is the leading cause of the disease. Most of the time the cause of childhood cancer is unknown, although genetic contributions related to overexpression or deletion of genes can be determined. On the other hand, adult cancers are frequently associated with alterations in the DNA (mutations) as well as lifestyle.
The treatment plays an important role in the differences between adult and childhood cancers. Usually, similar treatments are used for both adults and children, including chemotherapy, radiotherapy, surgery, transplants and immune therapy, according to the type of cancer and its stage. However, the doses and types of drugs may differ between them. The differences in the treatment go beyond the doses and encompass the mechanisms of action and possible long term toxicities of drugs. For example, the use of drugs that damage DNA can be prohibitive in children due to the increased risk of secondary cancers in the future.
In conclusion, specific types of cancer are more common in children and the cause of this disease is frequently unknown. Fortunately, children have great possibilities to survive cancers but the treatment needs to be carefully chosen and its long-term effect on the body have to be monitored for their whole life.
Written by Luiza Erthal
References
Kattner, P. et al. Compare and contrast: pediatric cancer versus adult malignancies. CancerMetastasis Rev. 38, 673–682 (2019).
Neuroblastoma relapse is one of the greatest challenges to complete cure for children with high-risk disease. At least 40% of high-risk neuroblastoma patients will experience cancer relapse 4 years after intense treatment, which includes a combination of chemotherapy, surgery, irradiation and the self-transplantation of stem cells (consolidation therapy).
To overcome this problem improved maintenance therapy is needed. These are therapies administered to patients after the end of the initial treatment to prevent tumour relapse. Frequently, maintenance therapy for neuroblastoma includes immunotherapies such as antibodies against GD-2 and cytokines and 13-cis-retinoic acid. Although these therapies have some positive effects, the rate of relapse is still high. Therefore, other options to prevent relapse are needed.
Recently, a phase II clinical trial evaluated the effect of Difluoromethylornithine (DFMO) on event-free survival (EFS) and overall survival (OS) of high-risk neuroblastoma patients1. Event-free survival means the length of time that the patient remains free of cancer after the end of treatment, while overall survival means the length of time that the patient is alive after the diagnosis or the start of treatment. The measurement of event-free survival and overall survival provides a good indication of the treatment effect.
In this clinical trial report the therapy efficacy on 81 patients that received immunotherapy treatment with dinutuximab and started DFMO maintenance therapy at least 120 days after completion of treatment were compared to the efficacy (based on medical records) from a group of 76 patients that got the same treatment but without the maintenance with DFMO.
DFMO inhibit the ornithine decarboxylase pathway, which is related to cell growth and decreased cell death, thus preventing cells to become cancerous and tumour progression. The results demonstrated that maintenance therapy with DFMO provided 85% of 5-year event-free survival compared to 65% for no-DFMO maintenance therapy, and 95% 5-year OS compared to 81% no-DFMO therapy2.
In conclusion, this study results suggest a benefit provided by the DFMO therapy in preventing neuroblastoma relapse. The researchers suggest that early therapy with DFMO may further improve these results. Therefore, more clinical trials evaluating this possibility are being conducted3,4.
Written by Luiza Erthal
References
1. SaulnierSholler, G. A Phase II Preventative Trial of DFMO (Eflornithine HCl) as a Single Agent in Patients With High Risk Neuroblastoma in Remission. https://clinicaltrials.gov/ct2/show/NCT02395666 (2020).
2. Lewis, E. C. et al. A subset analysis of a phase II trial evaluating the use of DFMO as maintenance therapy for high‐risk neuroblastoma. Int. J. Cancer 147, 3152–3159 (2020).
3. SaulnierSholler, G. Phase II Trial of Eflornithine (DFMO) and Etoposide for Relapsed/Refractory Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT04301843 (2021).
4. SaulnierSholler, G. NMTT- Neuroblastoma Maintenance Therapy Trial Using Difluoromethylornithine (DFMO). https://clinicaltrials.gov/ct2/show/NCT02679144 (2021).
Immunotherapies are treatments that stimulate the patient’s immune system to help it to fight cancer. This type of treatment is gaining more attention in neuroblastoma due to the possibility to combine it with other therapies, potentially, generating fewer side effects.
Clinical trials are research protocols performed in patients to evaluate whether a new treatment is safe and effective. This type of research can also compare standard treatments with new treatment options as well as investigate new combinations of drugs. Clinical trials occur in phases comprising phase I (safety), phase 2 (safety and efficacy), phase 3 (safety, efficacy and comparison with standard treatments for the specific disease).
According to a search performed on November 14th, 2021, there are 594 clinical trials for neuroblastoma at clinicaltrials.gov, a clinical trial database from the United States (US). From these, 173 are recruiting or active trials and 15 are related to immunotherapies. Generally, these are initial trials evaluating treatment combinations using chemotherapy, cell transplants and immunotherapy, including antibodies and vaccines.
Trials for antibodies
The most explored target for immunotherapy in neuroblastoma is the GD2, a molecule present in the surface of neuroblastoma cells that can be used to combat the tumour. Indeed, antibodies that bind to GD2 called dinutuximab and naxitamab are approved for use in the US to treat neuroblastoma1,2.
A clinical trial in the US and Canada is recruiting patients to evaluate the combination of dinutuximab with another antibody called Magrolimab in patients with neuroblastoma that do not respond to or come back after treatment3. This is an initial trial (Phase 1), which aims to determine the best doses and side effects of this combination.
Racotumomab, an antibody that binds to N-glycolyl GM3, a molecule that is highly expressed in the surface of neuroblastoma cells, is being evaluated in high-risk neuroblastoma5. The study aims to determine the immune response generated by the drug and the related toxicity.
Trials for vaccines
A trial from Dana-Farber Cancer Institute is recruiting patients to study the GVAX Vaccine and its combination with the antibodies, nivolumab and ipilimumab, that stimulates T-cells to attack the cancer 6. The vaccine is produced with neuroblastoma cells from the patient. The study will evaluate the dose and safety of the combination treatment.
Another trial is evaluating the use of a modified neuroblastoma cell vaccine in combination with low doses of chemotherapy (Cytoxan/Cyclophosphamide)7. A vaccination scheme comprising 8 doses of vaccine and cycles of oral chemotherapy is planned and patients will be closely monitored through the vaccination period to evaluate side effects and disease status. This study is ongoing and will follow the patients for 15 years after completing the vaccination scheme.
Trials for cell therapy
A trial evaluating the use of modified T-cells (CART-T-cell) to recognise GD2- neuroblastoma cells in combination with chemotherapies (cyclophosphamide and fludarabine) and an antibody (Pembrolizumab) is ongoing8. The combination is based on previous studies that have demonstrated the longer time presence of CAR T-cell in the blood of patients after intravenous infusion of chemotherapy. Moreover, the antibody will help to stimulate the patient immune system. The trial aims to determine the highest dose possible for the combination treatment generating fewer side effects.
Another Phase I immunotherapy trial for neuroblastoma aims to compare the treatment with dinutuximab and lenalidomide (drugs that support the immune system) and Natural Killer (NK) cells from the patient9. The NK cells can kill cancer cells while the two immunotherapeutic drugs activate the NK cells. This study will determine the safest dose of cells to be used in combination with the drugs.
Conclusion
Considering some of the clinical trials in progress that uses immunotherapy to treat neuroblastoma, we can conclude that this therapy modality holds great promise to advance and potentially serve as a new treatment option to improve neuroblastoma patients’ survival and quality of life.
Written by Luiza Erthal
References
1. Drugs Approved for Neuroblastoma – National Cancer Institute. https://www.cancer.gov/about-cancer/treatment/drugs/neuroblastoma (2011).
2. Memorial Sloan Kettering Cancer Center. Expanded Access Use of Naxitamab/GM-CSF Immunotherapy for Consolidation of Complete Remission or Relapsed/Refractory High-Risk Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT04501757 (2021).
3. National Cancer Institute (NCI). Phase 1 Trial of Hu5F9-G4 (Magrolimab) Combined With Dinutuximab in Children and Young Adults With Relapsed and Refractory Neuroblastoma or Relapsed Osteosarcoma. https://clinicaltrials.gov/ct2/show/NCT04751383 (2021).
4. Memorial Sloan Kettering Cancer Center. Hu3F8/GM-CSF Immunotherapy Plus Isotretinoin for Consolidation of First Remission of Patients With High-Risk Neuroblastoma: A Phase II Study. https://clinicaltrials.gov/ct2/show/NCT03033303 (2020).
5. Laboratorio Elea Phoenix S.A. Open-label, Multicenter, Phase II Immunotherapy Study With Racotumomab in Patients With High-risk Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT02998983 (2021).
6. Collins, N. B. A Phase 1 Study of Combination Nivolumab and Ipilimumab With Irradiated GM-CSF Secreting Autologous Neuroblastoma Cell Vaccine (GVAX) for Relapsed or Refractory Neuroblastoma. https://clinicaltrials.gov/ct2/show/NCT04239040 (2021).
7. Heczey, A. A Phase I/II Study Using Allogeneic Tumor Cell Vaccination With Oral Metronomic Cytoxan in Patients With High-Risk Neuroblastoma (ATOMIC). https://clinicaltrials.gov/ct2/show/study/NCT01192555 (2021).
8. Heczey, A. Autologous Activated T-Cells Transduced With A 3rd Generation GD-2 Chimeric Antigen Receptor And iCaspase9 Safety Switch Administered To Patients With Relapsed Or Refractory Neuroblastoma (GRAIN). https://clinicaltrials.gov/ct2/show/NCT01822652 (2021).
9. New Approaches to Neuroblastoma Therapy Consortium. A Phase I Dose Escalation Study of Autologous Expanded Natural Killer (NK) Cells for Immunotherapy of Relapsed Refractory Neuroblastoma With Dinutuximab +/- Lenalidomide. https://clinicaltrials.gov/ct2/show/NCT02573896 (2021).