Moving to a new country could be a challenge, an opportunity, or perhaps both. It involves stepping outside of your comfort zone, but that is where growth happens.
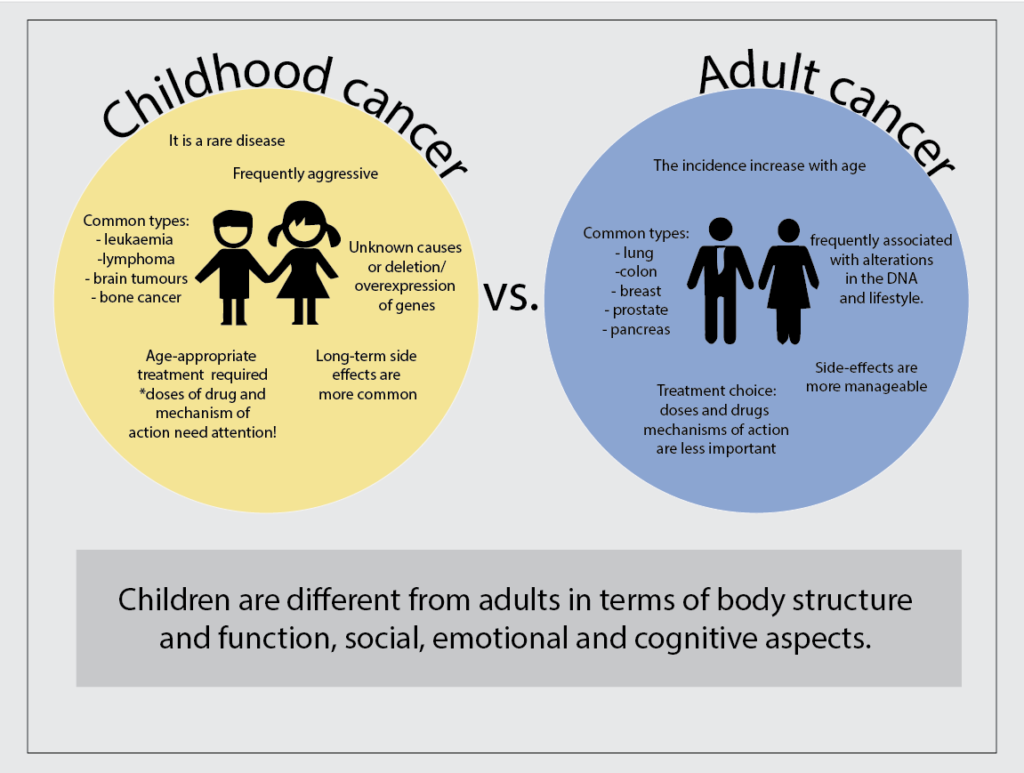
The most exciting opportunity of 2022 was my joining Dr Olga’s Lab as an MSc student. Welcome to the Research world full of uncertainty! Each day comes with a fresh set of surprises! Which is not uncommon in a lab environment. Sometimes things do not turn out the way we plan. But I am confident that every surprise will be worth it. My project contributes to the big ambition of Dr Olga’s team to develop an anti-cancer vaccine for children with neuroblastoma. It spans one year, which is rather short, but it gives me a fair impression of what a PhD journey might look like. I am already two months in, setting up my experiments, troubleshooting protocols and learning new things daily. Nevertheless, I enjoy that our team is outgoing, and I am eternally thankful to the whole team for their tremendous support and making me feel like I belong.

Outside of academics, I made a few adjustments. I got the chance to become acquainted with a new housing market, banking system, and visa administration as a non-Irish citizen. It seems simple, not really!
I also enjoy challenging my long-held beliefs. For instance, the after-work hangout and drinks is an intriguing example of a cultural difference I’ve noticed here. In Portugal, I used to enjoy my lab breaks with some pastel de nata with black coffee, but now I prefer a cup of butter h0t chocolate, which is everywhere.