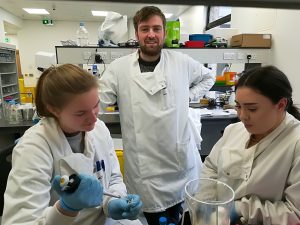
Last Friday we said Good Bye to 3 medical students who joined us to gain research experience. It has been quiet in the lab since they finished! It is always interesting to see their evolving journey as researchers.
“This research opportunity has given me the most exciting and rewarding experience during my undergraduate Medicine course. I got hands-on experience in ongoing medical research in Cancer biology which I think is unique of its kind for any undergraduate medical student. Throughout this journey, I could interact with many people coming from different domains including my collogues and my supervisor which giving me the opportunity to form professional relationships. I feel that my medical background helped me a lot along with my passion for the research work what I did in the lab. This research experience gave me an opportunity to gain and strengthen my skills like communication, time management, sincerity and judiciousness. I gained academic skills like scientific writing and critical thinking. I got exposure to various scientific equipment which I think is quite a rare opportunity for any undergraduate medical student. Overall, I think that by committing myself to medical research has given me a chance to understand Medicine from a different angle which I feel is an amazing and accomplishing experience for a medical student like me.” Sanat Rashinkar
Lab breakfast
“I arrived to the lab on my very first day feeling a little bit nervous but excited at the same time. Firstly, my partner Sanat and I were given a safety introduction talk by Seamus, who seemed very strict in regard to the safety rules but also turned out to be very fun. We then met the team who we’d be working with: Dr Olga, John, Ciara, Catherine, Thomas… Everyone turned out to be very lovely and friendly, making you feel very comfortable in the workplace. I also enjoyed the fact that we’d go for breakfast all together every once in a while; this really makes you feel like a part of a big family. My project was about melanoma and required some training that had to be completed before I could start my actual work. At first, everything seemed quite simple, however, when I started my actual research some things didn’t turn out as nicely as I expected. I mainly struggled with the microscope but Ciara was very patient with me and would give me a hand whenever I struggled. Overall, it was a very pleasant experience that gave me a great perspective into research, working alongside my colleagues on something as important as cancer. I truly believe that anyone who gets a chance to participate in research should really go for it as it makes you look at science differently and can also be fun.” Evgeniia Mustafaeva
Exciting times ahead for my team – to study neuroblastoma – immune cells interaction. This 3 years project is funded by Neuroblastoma UK to support the interdisciplinary collaboration between experts in fields of neuroblastoma biology, immunology and tissue engineering from Royal College of Surgeons in Ireland, Trinity College Dublin and Queen Mary University London.
Catherine Murphy, a new PhD candidate funded by Neuroblastoma UK
Catherine will grow different neuroblastoma cells together with immune cells using a 3D printing technology. She will travel to Queen Mary University London and learn how to do 3D tumour bioprinting. This technology allows the generation of reproducible scaffolds that replicate the architecture of tumour tissues as seen in patients. She will use RCSI/AMBER facilities to optimise this model here and to study how immune cells recognise cancer cells, attack and eventually kill them. This experimental model will help us to advance current immunotherapies and develop more effective treatments for neuroblastoma.
Here, we are – the Irish neuroblastoma research team landed at the 5th Neuroblastoma Research Symposium in Cambridge. Four poster presentations by four enthusiastic scientists. The two days crash course in neuroblastoma – vibrant, intense, informative.
I had one of the most enjoyable poster sessions in the last few years! A genuine interest in our 3D in vitro cancer models by both academics and Industry. Hope, to keep the ball rolling and strengthen these new links.
The Symposium programme was an excellent balance of the new transnational outcomes with hardcore developmental cellular programmes. From ‘How neuronal precursors select their fate and how they can escape the developmental constraints? How this knowledge can help to advance our understanding of neuroblastoma aetiology?’ to ‘New drugs that demonstrated great potency in pre-clinical studies’ via ‘how we can work together more efficiently to progress quicker’
Indeed, the success of the research meeting became possible thanks to the strategic vision and leadership of organisers!
13:00 – 13:10 Introduction – Neuroblastoma UK & CRUK Cambridge Centre
Session 1: Neuroblastoma biology & prognosis
Cancer Research UK Cambridge Centre Neuro-oncology Programme Session
Chair: Kate Wheeler (Oxford Children’s Hospital)
13:10 – 13:40 Sandra Ackermann (Cologne): The genetic basis of favourable outcome and fatal tumour progression in neuroblastoma
13:40 – 14:10 Rogier Versteeg (Amsterdam): The dark side of neuroblastoma
14:10 – 14:40 Katleen de Preter (Ghent): Improved diagnosis and risk stratification of paediatric cancers using liquid biopsies
14:40 – 14:55 Sue Burchill (Leeds): Self-renewing neuroblastoma cells isolated from bone marrow aspirates of children with stage M disease share a mesenchymal expression signature: an NCRI CCL CSG Neuroblastoma Group Study
14:55 – 15:15 Combined discussion
15:15 – 15:45 Tea with Posters
Session 2: Targeted & combination therapy I
Cancer Research UK Cambridge Centre Neuro-oncology Programme Session
Chair: Marie Arsenian Henriksson (Karolinska)
15:45 – 16:15 Frank Westermann (Heidelberg): Novel metabolic dependencies of MYCN-driven neuroblastoma
16:15 – 16:45 Gerard Evan (Cambridge): Is Myc really master of the universe?
16:45 – 17:00 Melinda Halasz (University College Dublin): Anti-Cancer Effects of Diphenyleneiodonium Chloride (DPI) In MYCN-Amplified Neuroblastoma
17:00 – 17:15 Evon Poon (ICR, Sutton): Pharmacological blockade of high-risk MYCN driven neuroblastoma using an orally-bioavailable CDK2/9 inhibitor
17:15 – 17:35 Combined discussion
Downing College – Main Hall.jpg
17:35 – 19:15 Poster viewing & Drinks
19:30 Symposium Dinner at Downing College (map for dinner)
FRIDAY 12TH APRIL 08:30 – 08:50 Coffee & pastries
Session 3: Neural crest & differentiation therapy I
Chair: Margareta Wilhelm (Karolinska)
08:50 – 09:20 Igor Adameyko (Karolinska): Normal development of sympathoadrenal system resolved with lineage tracing and single cell transcriptomics
09:20 – 09:50 Quenten Schwarz (Adelaide): Guiding sympathoadrenal neural crest cells to the adrenal primordia
09:50 – 10:05 Claudia Linker (King’s College London): Notch coordinates cell cycle progression and migratory behaviour leading to collective cell migration
10:05 – 10:20 Combined discussion
10:20 – 10:50 Coffee with Posters
Session 4: Neural crest & differentiation therapy II
Chair: Gareth Evans (York)
10:50 – 11:20 Karen Liu (King’s College London): ALK and GSK3 – shared features of neuroblastoma and neural crest
11:20 – 11:35 Anestis Tsakiridis (Sheffield): Efficient generation of trunk neural crest and sympathetic neurons from human pluripotent stem cells via a neuromesodermal progenitor intermediate
11:35 – 12:05 Anna Philpott (Cambridge): Using developmental mechanisms to drive differentiation of neuroblastoma
12:05 – 12:20 Combined discussion
12:20 – 13:20 Lunch with Posters
Session 5: Targeted & combination therapy II
Chair: Bengt Hallberg (Gothenburg)
Cancer Research UK Cambridge Centre Paediatrics Programme Lecture:
13:20 – 13:50 Sharon Diskin (Philadelphia): A multi-omic surfaceome study identifies DLK1 as a candidate oncoprotein and immunotherapeutic target in neuroblastoma
13:50 – 14:05 Donne Nile (Glasgow): Manipulation of cancer cell metabolism for neuroblastoma combination therapy with targeted radiotherapy
14:05 – 14:35 Suzanne Turner (Cambridge): CRISPR-dCas9 screens to identify resistance mechanisms to ALK in neuroblastoma
14:35 – 14:50 Combined discussion
14:50 – 15:20 Tea with Posters
15:20 – 15:30 Poster prizes
Session 6: Targeted & combination therapy III
Chair: John Lunec (Newcastle)
15:30 – 16:00 Per Kogner (Karolinska): The PPM1D encoded WIP1 phosphatase is an oncogene significant for cancer development and tumour progression and a druggable therapy target in neuroblastoma and medulloblastoma. A hint as to how aggressive childhood cancer manages with wild-type p53
16:00 – 16:15 Deb Tweddle (Newcastle): Preclinical assessment of MDM2/p53, ALK and MEK inhibitor combinations in neuroblastoma
16:15 – 16:30 Sally George (ICR, Sutton): A CRISPR-Cas9 genomic editing and compound screening approach identifies therapeutic vulnerabilities in the DNA damage response for the treatment of ATRX mutant neuroblastoma
16:30 – 16:45 Miriam Rosenberg (Jerusalem): Expression- and immune-profiling of neuroblastoma-associated Opsoclonus Myoclonus Ataxia Syndrome (OMAS) to identify features of auto- and tumour-immunity
Can you control the time? I can’t and know none who can. It flies, when things around you work out, and drags on when not. The time flies for me here in Baltimore. It feels so intense sometimes and then slightly slows down. I take pictures almost of everything: the path’s signposts when rambling in the network of Johns Hopkins Buildings, the first frosty morning, joyful deer at the backyard of my host family house, outdated clothes in the shop…
In the past, I had a similar journey to Ireland. It was 3 months research placement during my PhD. Did I like it – oh, yes I did! I travelled a lot, felt romantic and changed my life on my return home. But I did not run a diary or tag my way on Facebook. I have learnt the lesson: do it even more intense as you can’t travel back in time and write down your experience. It may be funny or educational to read in a couple of years! I become addicted to it though not always have time to do it.
I like the people who I am working with. They are a fantastic bunch of self-motivators and open-minded personalities. They are workaholics either naturally like me or because of the exciting projects they do like I do. Who knows, but very likely because of both. Isn’t it a dream to have an exciting project and great people around you? The luck like this gives you wings.
The American enthusiast studying Russian and my Mum
The host family – is my other great luck! This luck was crafted as a parallel story when none knew how the Fulbright application and an American enthusiast learning Russian may intersect. You would not believe, but parallel lines can be non-parallel sometimes! His journey to my home city in Russia paved the way to the opportunity to stay at his aunt’s house.
Every day 50 min drive to and from Hopkins opens up the other side of the local lifestyle and infrastructure. What are the rush hours? How many drivers are signalling before taking a turn? How do they call the shopping trolley? How parking system works?
Experiencing life as an American working in Baltimore.
Last year I have selected this photo of a lovely fountain capturing 3 girls under umbrellas (Drei-Mädchen-Brunnen) in Ballplatz Mainz in support of #ChildhoodCancerAwarnessMonth. This fountain was built between two Catholic girl’s schools symbolising the separate education and a happy childhood. It is charming on its own. And I’ve select it again.
Every child deserves a happy childhood. Raising awareness about childhood cancer we help to make the dreams of children with cancer come true. Dreams for a happy childhood, better treatment, better quality of life full of love ahead through better funding of childhood cancer research and access to innovative treatments.
Today marks the start of Childhood Cancer Awareness Month.
Three girls fountain in Mainz Germany
The cause of childhood cancers is believed to be due to faulty genes in stem cells that give rise to nerves, skin, blood and other body tissues. For some unknown reasons, the faulty genes can sit quiet and show their ‘bad’ character after birth and programme the cells into cancer cells.
So, there is no evidence that links lifestyle or environmental risk factors to the development of childhood cancer, which is opposite to many adult’s cancers.
Every 100th cancer patient is a child. Cancer is the 2nd most common cause of death among children after accidents.
Children are not little adults and so their cancer. Some childhood cancers have a good outlook and successful protocol of treatments. However, some of the cancers do not respond to the known drugs, or if respond cancer cells find the way to develop resistance and come back being more aggressive. Among theme are some forms of brain tumours, neuroblastoma and sarcomas; cancers developing in certain age groups and/or located within certain sites in the body, along with acute myeloid leukaemia (blood cancer). Children with a rare brain cancer – diffuse intrinsic pontine glioma survive less than 1 year from diagnosis. Children with soft tissue tumours have 5-year survival rates ranging from 64% (rhabdomyosarcoma) to 72%(Ewing sarcoma). Less than50% of children with the aggressive form of neuroblastoma will live beyond 5 years with current treatment strategies.
For majority of children who do survive cancer, the battle is never over. Over 60% of long‐term childhood cancer survivors have a chronic illness as a consequence of the treatment; over 25% have a severe or life-threatening illness.
The most common types of childhood cancer are:
Leukaemia and lymphoma (blood cancers)
Brain and other central nervous system tumours
Muscle cancer (rhabdomyosarcoma)
Kidney cancer (Wilms tumour)
Neuroblastoma (tumour of the non-central nervous system)
Bone cancer (osteosarcoma)
Testicular and ovarian tumours (gonadal germ cell tumours)
When I look back at the end of July, I am always surprised how quickly 8 summer weeks passed by. Summer students usually come very shy and uncertain and then they are flying through many complicated research terms and techniques. We help them to learn and they pay back by fantastic enthusiasm, commitment, and hard work. This summer was the same!
One of our experiences was donut’s tasting. We tasted donuts from Boston Donuts, the Rolling Donut, Boomerang Donuts and Krust Bakery. Many shapes, textures, and tastes. Krust Bakery did our favourites. 🙂
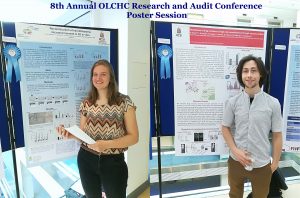
This was our 2nd time attending the OLCHC Research & Audit Day on May 25th, 2018. The conference provides a great forum for paediatric clinicians to share and update knowledge across different specialties through talks and poster presentations. It is insightful for basic biomedical researchers like us to see other perspectives.
I was delighted to know that two our studies were shortlisted. It is a rewarding feeling to see your Dream Team doing very well. One was the project of the Erasmus+ student Hanne Pappaert and the other was the project of NCRC funded Postdoc John Nolan. Hanne explored our 3D tissue-engineered model of neuroblastoma using collagen-based scaffolds with distinct mechanical properties. These new scaffolds were designed and manufactured by our collaborator Dr Cian O’Leary from Pharmacy Department and Tissue Engineering and Research Group (TERG) headed by Prof Fergal O’Brien. Hanne grew 5 neuroblastoma cell lines on the 3 scaffolds: hard like a rock, soft and fluffy like a cotton wool and a jelly-like. All cells liked the jelly-like environment. This environment is similar to bone marrow – the most common site of neuroblastoma metastasis. We were excited to see the difference as it means we are one step closer to reconstruct this type of tumour spread.
John has expanded our exploration of our 3D neuroblastoma model by examining the content of exosomes – little parcels sent by cancer cells in 3D and as tumours grown in mice. We were thrilled to see a high similarity in the exosomal content. This finding additionally proved the great applicability of our 3D model as a tool to study neuroblastoma.
Though the official announcement is scheduled for the first week of June, the groundwork is on. Lots of reading and planning for the trip to Johns Hopkins later this year. One of the first is the book by Rebecca Skloot ‘The Immortal Life Of Henrietta Lacks”. The famous HeLa cells were generated by researchers at JH. The story is a fascinating journey for biomedical scientists and a tragedy for the Lacks family.
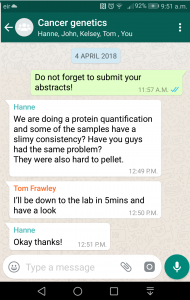
Here is the perfect example of the teamwork troubleshooting protein extractions. My Dream Team 2018 in action. The current information and communication technologies allow to stay connected and respond quickly.
Five minutes later in the lab: troubleshooting is the exchange of experiences!








 This was our 2nd time attending the OLCHC Research & Audit Day on May 25th, 2018. The conference provides a great forum for paediatric clinicians to share and update knowledge across different specialties through talks and poster presentations. It is insightful for basic biomedical researchers like us to see other perspectives.
This was our 2nd time attending the OLCHC Research & Audit Day on May 25th, 2018. The conference provides a great forum for paediatric clinicians to share and update knowledge across different specialties through talks and poster presentations. It is insightful for basic biomedical researchers like us to see other perspectives.