Have you heard that ice cream consumption increases the number of shark attacks? Or that when Nicolas Cage appears in movies, the number of drowning cases goes up? Should we just ban ice cream and Nicolas Cage to avoid these tragedies… well, it is not as straightforward as that.
I discovered this topic of bizarre correlations during the first few weeks of the introduction to statistics module. They were quite fun to discuss, and we had a few laughs speculating how they were made in the first place. Here, I just wanted to share a couple of these bizarre correlations and touch upon broader implications.
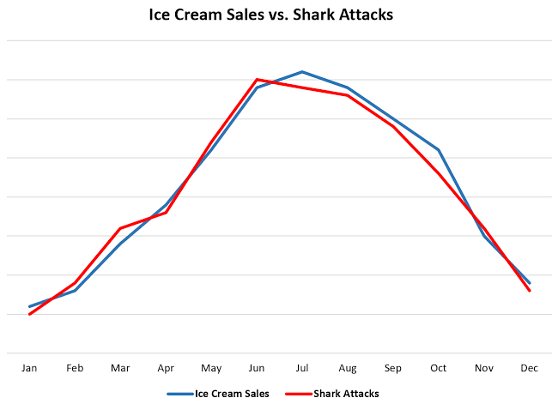
Just because two variables move together on a graph does not mean one causes the other. Shark attacks are not caused by eating more ice cream; both are connected (sharks and ice cream), but a third variable can lead to an increase in the summertime, when people go to the beach for a swim. Similarly, Nicolas Cage movies tend to be released in the summer, when people are more likely to drown. This is an example of confounding variables, where two variables seem to be connected (sharks and ice cream), but there is a third variable that is influencing both behind the scenes (summertime). People tend to forget that correlation does not imply causation, leading to hilarious or even dangerous misinterpretations of data.
In research, the idea of confounding effects is not as straightforward. For example, the more a person eats, the more sodium they consume, but also eating a lot of calories often leads to obesity. Both obesity and high-sodium diets are believed to correlate with high blood pressure. So, then what is the primary cause in this case: obesity or high sodium intake?
Tools like LASSO or Elastic Net can help tease apart which variable is really doing the work, but the data only goes so far. It still takes a researcher to interpret what it means. So the next time a striking statistic makes you want to ban ice cream (or Nicolas Cage), it’s worth pausing to wonder what’s really going on behind the scenes.
Written by Dmytro Brykaylo
Reference:
Correlation vs. Causation. Association of Health Care Journalists.
Nick Cage Movies Vs. Drownings, and More Strange (but Spurious) Correlations | National Geographic.
Siegel, E. Why Ice Cream Is Linked to Shark Attacks – Correlation/Causation Smackdown. KDnuggets.