

The determination of the tumour stage is an important step after a neuroblastoma diagnosis. The stage of neuroblastoma is determined depending on tumour location and if it has spread to other parts of the body. This will guide risk group assignment and treatment choice.
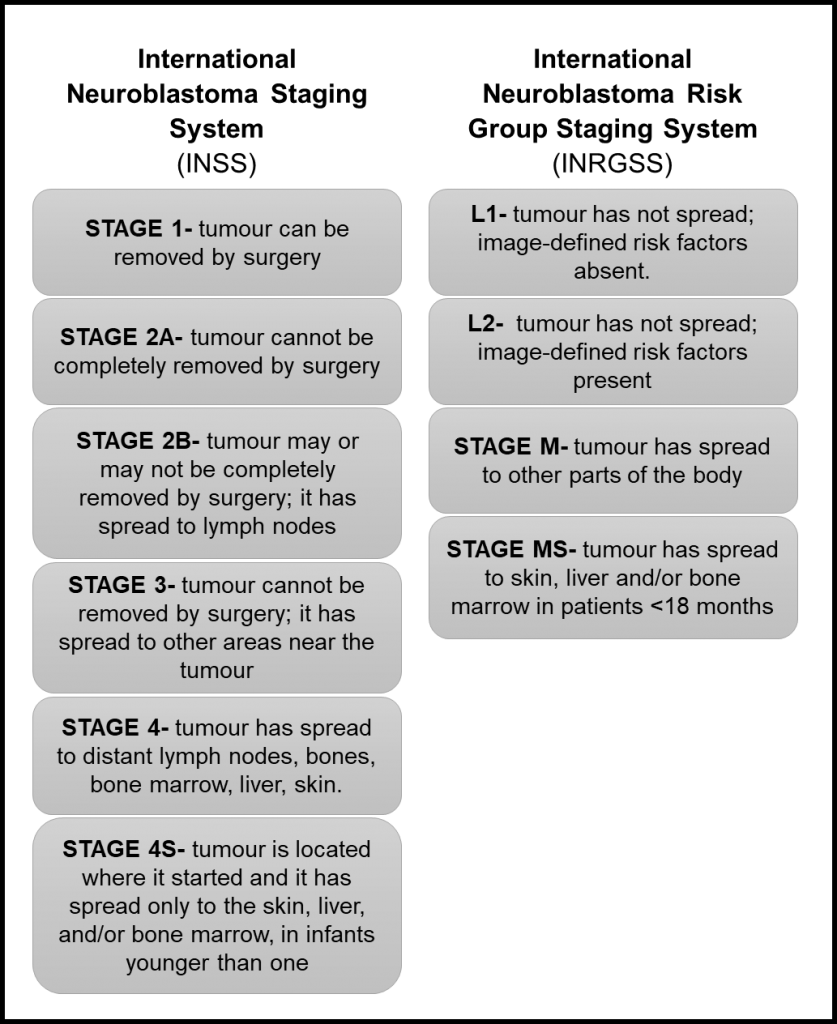
The first staging system for neuroblastoma, the International Neuroblastoma Staging System (INSS), was developed in 1986 and is based on the pathological evaluation of the tumour after a removal surgery. In 2005, The International Neuroblastoma Risk Group Staging System (INRGSS) started to be used. This system is based on tumour images before any surgery. Therefore, it is based on image-defined risk factors to determine the tumour stage (see table below). It also uses clinical, pathologic, and genetic markers to determine the risk groups, which can be low-risk, intermediate-risk, or high-risk.
Reference: Neuroblastoma – Childhood: Stages and Groups, Cancer.net.
Recently, the Children’s Oncology Group (COG), a clinical trial group dedicated to paediatric cancer research revised the classification system they use to determine tumour stage for enrolment in clinical trials1. Previously, they have been defining the tumour stage based on the INNS system. Now they proposed a revised classification that takes into account the INRGSS and chromosomal alterations.
Key clinical and biological factors used in the neuroblastoma risk classification include age at diagnosis, disease stage, tumour tissue appearance under a microscope (histology), the status of the gene MYCN that affects tumour growth, the amount of DNA in a tumour cell (called tumour cell ploidy), and alterations in the DNA.
They analyse the outcome of almost 5,000 patients to define risk groups based on the INRGSS, using alterations in the DNA of tumour cells as a biomarker and considering current therapy modalities. In general, they found that the correlation of stages between systems is not exact. However, the differences in survival were minimal when comparing staging systems, which corroborates the use of the revised version.
In general, the new version classifies L1 and L2 tumours as low risk, except for L1 tumours with alteration in the gene MYCN and that cannot be removed by surgery, which is high-risk. For L2 tumours, MYCN status and age can be used to evaluate prognosis. Stage M tumours can be classified as high risk or intermediate-risk depend on age, MYCN status and DNA alterations. In conclusion, low-risk groups have excellent outcomes with any or limited therapy, the intermediate-risk group have very good outcomes and high-risk groups have inferior outcomes despite therapy.
This new version of the COG classifier will provide a uniformization of patient risk classification for clinical trials, ultimately enabling the comparison between different trials.
Written by Luiza Erthal
Reference:
1. Irwin, M. S. et al. Revised Neuroblastoma Risk Classification System: A Report From the Children’s Oncology Group. J. Clin. Oncol. JCO.21.00278 (2021)