References:
Gatta G, Botta L, Rossi S, Aareleid T, Bielska-Lasota M, Clavel J, et al. Childhood cancer survival in Europe 1999-2007: Results of EUROCARE-5-a population-based study. Lancet Oncol. 2014;15(1):35–47.
Ward E, Desantis C, Robbins A, Kohler B, Jemal A. Childhood and Adolescent Cancer Statistics, 2014. Ca Cancer J Clin. 2014;64(2):83–103.
Dolgin MJ, Jay SM. Childhood cancer. 1989;327–40.
Miller RW, Young Jr. JL, Novakovic B. Childhood cancer. Cancer [Internet]. 1995;75(1 Suppl):395–405.
Raab CP, Gartner JC. Diagnosis of Childhood Cancer. Primary Care – Clinics in Office Practice. 2009. p. 671–84.
Howlader N, Noone A, Krapcho M, Garshell J, Miller D, Altekruse S, et al. SEER Cancer Statistics Review, 1975-2011 [Internet]. National Cancer Institute. 2014.
Ries L a. G, Smith M a., Gurney JG, Linet M, Tamra T, Young JL, et al. Cancer incidence and survival among children and adolescents: United States SEER Program 1975-1995. NIH Pub No 99-4649. 1999;179 pp
Warren KE. Diffuse intrinsic pontine glioma: poised for progress. Front Oncol [Internet]. 2012;2(December):205.
Lackner H, Benesch M, Schagerl S, Kerbl R, Schwinger W, Urban C. Prospective evaluation of late effects after childhood cancer therapy with a follow-up over 9 years. Eur J Pediatr. 2000;159(10):750–8.
Mission
To increase the understanding of neuroblastoma pathogenesis,
progression and treatment failure and to improve survival
and quality of life for children with neuroblastoma.
Main Objectives
To consolidate a platform for global collaboration
To establish networks of multidisciplinary caregivers
To develop new trial protocols
To develop standards for radiotherapy and surgery
To develop SOPs for biomaterial collection, handling and storage
To develop SOPs for application of major research technologies
There is no short answer. Research is a slow, meticulous process of testing theories and finding out which ones work.It is exactly the same for both curiosity- and disease- driven questions. Long years of ground research full of ups and downs are critical for any breakthrough or progress. Very often with more downs than ups. Importantly, all researchers build on the work of their predecessors. This is the nature of science.
To understand the world around us, we have to do be curious and do “blue sky or curiosity-driven” research. It is a long shot, but this type of research can lead to practical applications down the road. One of the most recent examples is a drug Vismodegib (Erivedse) to treat basal cell carcinoma (the most common type of skin cancer) approved by the FDA in 2012. This drug targets genes of a hedgehog-associated signalling pathway. Defects in this pathway were found to drive many cases of skin cancer. But, how this relationship was found? Blue sky research!
Researchers studied hedgehog signalling in fruit flies and mice. One of the researchers had a strong interest in a fruit fly gene called hedgehog. If this gene is defective, then fly embryos look stubby and hairy aka a hedgehog. Further research brought more interesting facts and relationships leading to the identification of a drug that can stop the function of this faulty gene. Decades later with the advancement of genome sequencing, the defect in hedgehog signalling pathway genes was identified in patients with locally advanced and metastatic basal cell carcinoma.
What would happen if there were no research in fruit flies and mice? There would have been no rationale to create a drug like Vismodegib!
The best discovery research is unrestricted. It is driven by intellectual curiosity and conceptual advancement. More such curiosity- driven research is needed. For every medical breakthrough, for every Vismodegib, there were hundreds of blind alleys and failed ideas.
The research is a long-term investment. This contradicts to the short-term life of the politicians and governments who give the money. They do not take the risks. So, the discovery research becomes critically underfunded.
Fundraising creates opportunities for blue sky research and developing cancer treatments.
Thank you all who support cancer research charities!
This is the first time in the history of the IACR meetings when an entire plenary session is solely dedicated to challenges and advancements in childhood cancer.
This session will unite Internationally recognised leaders in childhood cancer research. They will speak about what we know about origin and evolution of childhood cancers (Prof. Tariq Enver), how blood biomarkers can help in stratification and treatment of children (Prof. Sue Burchill), what impact Down syndrome has in the white blood cell cancer development and progression (Prof. Irene Roberts), how epigenetic changes affect tumour pathogenesis and future of therapeutics targeting theses changes (Prof Raymond Stallings).
Today, we are celebrating International Childhood Cancer Day to raise awareness and to express support for children and adolescents with cancer, survivors and their families.
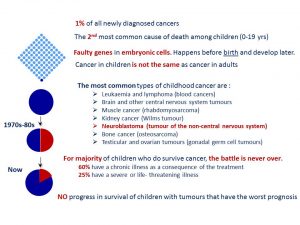
Childhood cancer is an umbrella term for a great variety of malignancies which vary by site of disease origin, tissue type, race, sex, and age.
The cause of childhood cancers is believed to be due to faulty genes in embryonic cells that happen before birth and develop later. In contrast to many adult’s cancers, there is no evidence that links lifestyle or environmental risk factors to the development of childhood cancer.
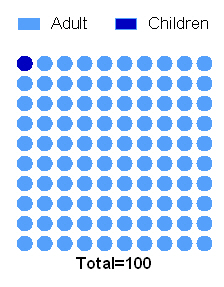
Every 100th patient diagnosed with cancer is a child.
In the last 40 years the survival of children with most types of cancer has radically improved owing to the advances in diagnosis, treatment, and supportive care. Now, more than 80% of children with cancer in the same age gap survive at least 5 years when compared to 50% of children with cancer survived in 1970s-80s.
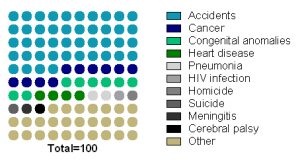
Childhood cancer is the second most common cause of death among children between the ages of 1 and 14 years after accidents.
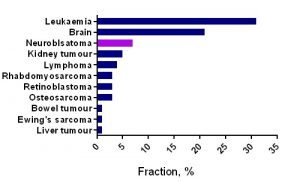
Unfortunately, no progress has been made in survival of children with tumours that have the worst prognosis (brain tumours, neuroblastoma and sarcomas, cancers developing in certain age groups and/or located within certain sites in the body), along with acute myeloid leukaemia (blood cancer). Children with a rare brain cancer – diffuse intrinsic pontine glioma survive less than 1 year from diagnosis. Children with soft tissue tumours have 5-year survival rates ranging from 64% (rhabdomyosarcoma) to 72% (Ewing sarcoma).
For majority of children who do survive cancer, the battle is never over. Over 60% of long‐term childhood cancer survivors have a chronic illness as a consequence of the treatment; over 25% have a severe or life‐ threatening illness.
This post is dedicated to parents of children with neuroblastoma. Some parents asked about DFMO – a re-purposing drug. In this post, I tried to collect and summarize information available from academic sources.
Q1: What is DFMO?
Difluoromethylornithine (DFMO, Eflornithine) is an anti-protozoan drug. It was originally developed and FDA approved for the treatment of Trypanosoma brucei gambiense encephalitis (“African sleeping sickness”). DFMO permanently binds to ornithine decarboxylase (ODC), an important enzyme in polyamine metabolism, and prevents the natural substrate ornithine from entering the active site.
By inhibiting ODC, DFMO reduces cellular polyamines and inhibits cell growth and proliferation of actively dividing cells, thus making DFMO an attractive candidate for cancer therapy. In neuroblastoma, a positive regulation of all aspects of polyamine metabolism by MYCN was reported (revived by Bassiri 2015, Gamble 2012). So, it is believed that MYCN amplified neuroblastomas would most benefit of the drug.
Q2: How intense is basic science behind DFMO in neuroblastoma?
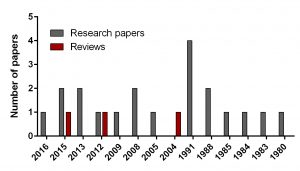
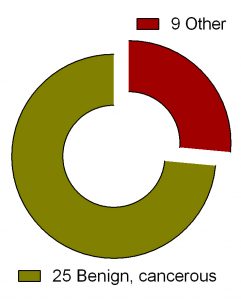
Figure 1. Breakdown of papers covering DFMO in neuroblastoma
To find out the intensity of basic science on DFMO in neuroblastoma search for ‘difluoromethylornithine/DFMO/Eflornithine’ and ‘neuroblastoma’ was run in PubMed, a web-based resource with 26 million citations for biomedical literature from MEDLINE, life science journals, and online books. The search returned 23 papers including 3 reviews and 20 primary research reports published from 1980 to present.
In comparison, I did another search for a novel drug Unituxin (dinutuximab) approved by FDA in 2015. It is monoclonal antibody against the glycolipid disialoganglioside GD2, a biomarker specific for neuroblastoma. Search for ‘anti-GD2 antibody’ and ‘neuroblastoma’ returned 181 papers including 25 reviews and 156 primary articles for the same period.
Q3: Is DFMO in cancer clinical trials?
“ClinicalTrials.gov is a Web-based resource that provides patients, their family members, health care professionals, researchers, and the public with easy access to information on publicly and privately supported clinical studies on a wide range of diseases and conditions. The Web site is maintained by the National Library of Medicine (NLM) at the National Institutes of Health (NIH).
Figure 2. Clinical trials of DFMO in various health conditions.
Search for ‘difluoromethylornithine/DFMO/Eflornithine’ in ClinicalTrials.gov returned 36 registered trials across different health conditions.Two of these were withdrawn, the breakdown for the rest 34 is as follows: Adenomatous Polyp (1), Anaplastic Astrocytoma/Recurrent Anaplastic Astrocytoma (1), Bladder Cancer (1), Cervical Cancer/Precancerous Condition (1), Colorectal Cancer (3), Esophageal Cancer (1), Familial Adenomatous Polyposis (1), Gastric Cancer/Gastric Intestinal Metaplasia (1), Hirsutism (2), Human African Trypanosomiasis (5), Neuroblastoma (7), Non-melanomatous Skin Cancer/Precancerous/Nonmalignant Condition (4), Post-solid Organ Transplant/Skin Neoplasms (1), Precancerous Condition (1), Prostate Cancer (2), Pseudofolliculitis Barbae (1), Type 1 Diabetes (1) (Fig. 2). To see full details of 34 trials please click at this Table.
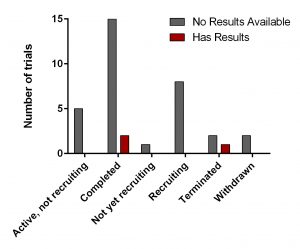
Figure 3. DFMO clinical trials from ClinicalTrials.gov
All of them have various statuses (Fig. 3) as well as study design. Importantly, 30 out of 34 studies are focused on safety and efficacy of this drug. Vast majority of studies of DFMO in adult cancers/benign conditions are randomized (16/18 or 89%). Randomization in assignment of patients in studied groups (control and new drug/combination) helps minimize researcher’s bias when comparing effect of the new treatment vs current/no treatment. All trials of DFMO in neuroblastoma are not randomized. Instead, studies use a single group assignment.
Three trails have been either completed/terminated and published results are available at ClinicalTrials.gov (NCT01059071, NCT00033371. NCT00118365).
Q4: What about clinical trials of DFMO in neuroblastoma?
The trial NCT01059071 was a Phase 1 clinical trial. A phase I clinical trial tries to find out whether a new treatment/drug is safe, what its side effects are, the best dose of the new treatment, if the treatment shrinks the cancer.
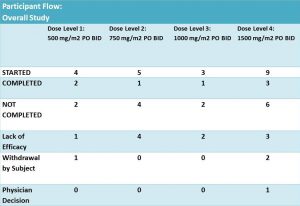
Twenty one patients were enrolled and eligible for treatment with DFMO and DFMO + etoposide. These patients were assigned into 4 groups of different DFMO doses (Fig. 4). The treatment was in cycles of 21 days. Cycle 1 – DFMO only followed by cycle 2 – combined treatment of DFMO+etoposide (14 days) and DFMO only (the last 7 days).
Figure 4. Table was adopted from results section of the clinical trial NCT01059071
According to results of the trial: 14 patients did not complete the treatment due to different reasons. It was not clear what stage/cycle they left the trial.
As mentioned earlier this study used a single group assignment and a design called ‘3+3’. This design is straightforward and safe. Briefly, it means that for a dose (X) of the drug, 6 patients are selected. Of these, 3 receive the dose X and are monitored for a period of time. If no adverse effects are registered in these 3, then another new 3 patients start the same treatment. The effect of the drug is evaluated on the patent’s health condition before-, during – the treatment and after its completion. This approach is often used in vaccine tests and dose escalation methods in Phase I cancer clinical trials. This type of study can answer mainly two questions: 1) whether the tested drug is safe to use and 2) what doses are safe? The main drawbacks of this design are
Many patients treated at doses below therapeutic effect
Slow dose increase
Uncertainty about the recommended phase II dose (RP2D)
Only the result from the current dose is used for determining the dose of next cohort of patients. Information on other doses is ignored
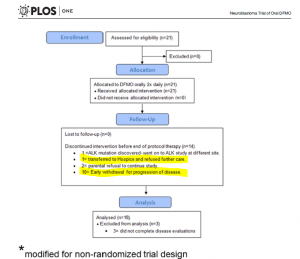
Figure 5 is adopted from Sholler GL et al, PLoS One. 2015 May 27;10(5):e0127246.
Q6: What are main findings of the clinical trial NCT01059071?
The overflow of the study is presented in Fig 5 providing additional information on those who did not complete the trial. Out of 14 participants, disease has progressed in 11 patients – it is 52% of the enrolled participants. Authors highlighted that this phase I study was not designed to evaluateanti-tumour efficacy of DFMO. But tumour response and clinical response were monitored during the study.
According to the paper, 21 patients received at least one dose of DFMO only (Cycle 1, 21 days). During this cycle, 3 patients were withdrawn. All of them were assessed for safety of DFMO.
Eighteen of them completed cycle 1 and continued treatment with DFMO+etoposide for another 4 cycles followed with DFMO only therapy for a number of cycles. Their clinical response data were examined for efficacy of DFMO alone.
Three out of 21 participating patients in this clinical trial remain alive and disease free between 2–4.5 years after starting DFMO.
Authors concluded that
DFMO doses of 500-1500mg/m2/day are safe and well tolerated in children with relapsed NB
Research and review papers covering DFMO in neuroblastoma:
Evageliou NF, Haber M, Vu A, Laetsch TW, Murray J, Gamble LD, Cheng NC, Liu K, Reese M, Corrigan KA, Ziegler DS, Webber H, Hayes CS, Pawel B, Marshall GM, Zhao H, Gilmour SK, Norris MD, Hogarty MD. Polyamine Antagonist Therapies Inhibit Neuroblastoma Initiation and Progression. Clin Cancer Res. 2016 Sep 1;22(17):4391-404. doi: 10.1158/1078-0432.CCR-15-2539.
Bassiri H, Benavides A, Haber M, Gilmour SK, Norris MD, Hogarty MD. Translational development of difluoromethylornithine (DFMO) for the treatment of neuroblastoma. Transl Pediatr. 2015 Jul;4(3):226-38. doi: 10.3978/j.issn.2224-4336.2015.04.06. Review.
Saulnier Sholler GL, Gerner EW, Bergendahl G, MacArthur RB, VanderWerff A, Ashikaga T, Bond JP, Ferguson W, Roberts W, Wada RK, Eslin D, Kraveka JM, Kaplan J, Mitchell D, Parikh NS, Neville K, Sender L, Higgins T, Kawakita M, Hiramatsu K, Moriya SS, Bachmann AS. A Phase I Trial of DFMO Targeting Polyamine Addiction in Patients with Relapsed/Refractory Neuroblastoma. PLoS One. 2015 May 27;10(5):e0127246. doi: 10.1371/journal.pone.0127246.
Lozier AM, Rich ME, Grawe AP, Peck AS, Zhao P, Chang AT, Bond JP, Sholler GS Targeting ornithine decarboxylase reverses the LIN28/Let-7 axis and inhibits glycolytic metabolism in neuroblastoma. Oncotarget. 2015 Jan 1;6(1):196-206.
Samal K, Zhao P, Kendzicky A, Yco LP, McClung H, Gerner E, Burns M, Bachmann AS, Sholler G. AMXT-1501, a novel polyamine transport inhibitor, synergizes with DFMO in inhibiting neuroblastoma cell proliferation by targeting both ornithine decarboxylase and polyamine transport. Int J Cancer. 2013 Sep 15;133(6):1323-33. doi: 10.1002/ijc.28139.
Koomoa DL, Geerts D, Lange I, Koster J, Pegg AE, Feith DJ, Bachmann AS. DFMO/eflornithine inhibits migration and invasion downstream of MYCN and involves p27Kip1 activity in neuroblastoma. Int J Oncol. 2013 Apr;42(4):1219-28. doi: 10.3892/ijo.2013.1835.
Gamble LD, Hogarty MD, Liu X, Ziegler DS, Marshall G, Norris MD, Haber M. Polyamine pathway inhibition as a novel therapeutic approach to treating neuroblastoma. Front Oncol. 2012 Nov 16;2:162. doi: 10.3389/fonc.2012.00162. Review
Passariello CL, Gottardi D, Cetrullo S, Zini M, Campana G, Tantini B, Pignatti C, Flamigni F, Guarnieri C, Caldarera CM, Stefanelli C. Evidence that AMP-activated protein kinase can negatively modulate ornithine decarboxylase activity in cardiac myoblasts. Biochim Biophys Acta. 2012 Apr;1823(4):800-7. doi: 10.1016/j.bbamcr.2011.12.013.
Rounbehler RJ, Li W, Hall MA, Yang C, Fallahi M, Cleveland JL. Targeting ornithine decarboxylase impairs development of MYCN-amplified neuroblastoma. Cancer Res. 2009 Jan 15;69(2):547-53. doi: 10.1158/0008-5472.CAN-08-2968.
Koomoa DL, Yco LP, Borsics T, Wallick CJ, Bachmann AS. Ornithine decarboxylase inhibition by alpha-difluoromethylornithine activates opposing signaling pathways via phosphorylation of both Akt/protein kinase B and p27Kip1 in neuroblastoma. Cancer Res. 2008 Dec 1;68(23):9825-31. doi: 10.1158/0008-5472.CAN-08-1865.
Hogarty MD, Norris MD, Davis K, Liu X, Evageliou NF, Hayes CS, Pawel B, Guo R, Zhao H, Sekyere E, Keating J, Thomas W, Cheng NC, Murray J, Smith J, Sutton R, Venn N, London WB, Buxton A, Gilmour SK, Marshall GM, Haber M. ODC1 is a critical determinant of MYCN oncogenesis and a therapeutic target in neuroblastoma. Cancer Res. 2008 Dec 1;68(23):9735-45. doi: 10.1158/0008-5472.CAN-07-6866.
Wallick CJ, Gamper I, Thorne M, Feith DJ, Takasaki KY, Wilson SM, Seki JA, Pegg AE, Byus CV, Bachmann AS. Key role for p27Kip1, retinoblastoma protein Rb, and MYCN in polyamine inhibitor-induced G1 cell cycle arrest in MYCN-amplified human neuroblastoma cells. Oncogene. 2005 Aug 25;24(36):5606-18.
Bachmann AS. The role of polyamines in human cancer: prospects for drug combination therapies. Hawaii Med J. 2004 Dec;63(12):371-4. Review
Chen ZP, Chen KY. Differentiation of a mouse neuroblastoma variant cell line whose ornithine decarboxylase gene has been amplified. Biochim Biophys Acta. 1991 Dec 3;1133(1):1-8.
Piacentini M, Fesus L, Farrace MG, Ghibelli L, Piredda L, Melino G. The expression of “tissue” transglutaminase in two human cancer cell lines is related with the programmed cell death (apoptosis). Eur J Cell Biol. 1991 Apr;54(2):246-54.
Melino G, Piacentini M, Patel K, Annicchiarico-Petruzzelli M, Piredda L, Kemshead JT. Retinoic acid and alpha-difluoromethylornithine induce different expression of neural-specific cell adhesion molecules in differentiating neuroblastoma cells. Prog Clin Biol Res. 1991;366:283-91.
Stephanou A, Knight RA, De Laurenzi V, Melino G, Lightman SL.Expression of pre-opiomelanocortin (POMC) mRNA in undifferentiated and in vitro differentiated human neuroblastoma cell lines. Prog Clin Biol Res. 1991;366:173-80.
Melino G, Farrace MG, Ceru’ MP, Piacentini M. Correlation between transglutaminase activity and polyamine levels in human neuroblastoma cells. Effect of retinoic acid and alpha-difluoromethylornithine. Exp Cell Res. 1988 Dec;179(2):429-45.
Chen KY, Dou QP. NAD+ stimulated the spermidine-dependent hypusine formation on the 18 kDa protein in cytosolic lysates derived from NB-15 mouse neuroblastoma cells. FEBS Lett. 1988 Mar 14;229(2):325-8.
Karvonen E, Andersson LC, Pösö H. A human neuroblastoma cell line with a stable ornithine decarboxylase in vivo and in vitro. Biochem Biophys Res Commun. 1985 Jan 16;126(1):96-102.
Pösö H, Karvonen E, Suomalainen H, Andersson LC. A human neuroblastoma cell line with an altered ornithine decarboxylase. J Biol Chem. 1984 Oct 25;259(20):12307-10.
Chen KY, Nau D, Liu AY. Effects of inhibitors of ornithine decarboxylase on the differentiation of mouse neuroblastoma cells. Cancer Res. 1983 Jun;43(6):2812-8.
Chapman SK. Antitumor effects of vitamin A and inhibitors of ornithine decarboxylase in cultured neuroblastoma and glioma cells. Life Sci. 1980 Apr 21;26(16):1359-66. No abstract available.
SIOP is the International Society of Paediatric Oncology. It is a global multidisciplinary society representing doctors, nurses, other health care professionals, scientists and patients or their relatives. The Society’s motto is ‘no child should die of cancer’. The meeting 2017 is being held in Dublin, the city where I live and work.
Indeed, it was appealing to attend the key meeting in childhood oncology field. As any participant, I had an opportunity to submit an abstract about my research. To no surprise at all, I received email notifying me on my work being selected for e-Poster presentation. Common stuff. The email also said that it would be displayed at designated stations, like big screens throughout the meeting. Very unusual format, but we are living in the digital technology era; things are changing all the time. So, I would not need to stay by the poster this time. Great – more time for networking and talks.
Then I received another email informing about a Poster Discussion session, which I assumed to be a standard procedure when a group of selected piers stand by your poster and ask Qs. None comes in majority cases. A participant stands and waits and waits till the session is over. So, of course I took it easy.
A day before the meeting, I downloaded the meeting app and started to browse along the content and features. Out of curiosity, I checked details of the Poster Discussion session. This was the moment of mental breakdown – I discovered being selected for an oral poster presentation! My chances were 1 in 1475 (the number of submitted abstracts). I should probably also buy a lottery ticket tonight. Could lucky things come together?
I will reflect on the new e-poster presentation experience later today…




 This meeting is the biggest event for Irish cancer researchers.
This meeting is the biggest event for Irish cancer researchers.