To be able to guide the treatment of neuroblastoma patients, doctors have developed a number of classification systems. Although sharing common features, they slightly vary by medical center, country and continents making direct comparisons of treatment results difficult. Doctors and scientists are trying to consolidate all systems in one in order to evaluate treatments in the past, currently ongoing and in the future.
Scientists have suggested a newer risk group classification system, the International Neuroblastoma Risk Group (INRG) classification that would incorporate the best knowledge gained and recent advancements in the disease imaging and neuroblastoma molecular diagnostics. This system is based on imaging criteria using the image-defined risk factors (IDRFs) and the prognostic factors such as:
- The child’s age
- Tumour histology (the tumour appearance under the microscope)
- The presence or absence of MYCN gene amplification
- Certain changes in chromosome 11 (known as an 11q aberration)
- DNA ploidy (the total number of chromosomes in the tumour cells)
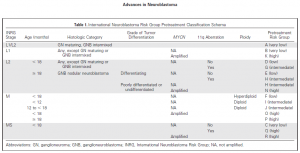
Using these factors the INRG classification put children into 16 different pre-treatment groups (lettered A through R). Each of these pretreatment groups is within 1 of 4 overall risk groups:
- Very low risk (A, B, C)
- Low risk (D, E, F)
- Intermediate risk (G, H, I, J)
- High risk (K, N, O, P, Q, R)
This system has not yet become common across all medical centers, but it is being researched in new treatment protocols.
Doctors and scientists are planning to improve the INRG classification system by incorporating other molecular diagnostics data such as profiles of the neuroblastoma genome (DNA), transcriptome (RNA), and epigenome* in order to make precise prognostication even better.
References:
Pinto NR, Applebaum MA, Volchenboum SL, Matthay KK, London WB, Ambros PF, Nakagawara A, Berthold F, Schleiermacher G, Park JR, Valteau-Couanet D, Pearson AD, Cohn SL. Advances in Risk Classification and Treatment Strategies for Neuroblastoma.J Clin Oncol. 2015 Sep 20;33(27):3008-17.


 This meeting is the biggest event for Irish cancer researchers.
This meeting is the biggest event for Irish cancer researchers.