7th OLCHC RESEARCH & AUDIT DAY Programme can be downloaded here Final Programme – OLCHC 2017


My WordPress Blog is about neuroblastoma biology and Cancer Bioengineering Group

The research is a long-term investment. It is always built up on the work of the predecessors. Keep research running is crucial to make the dreams come true. Dreams for better treatment options and quality of life.

Thank you to everyone involved in raising funds for CMRF!
CMRF Spring Newsletter can be found here – CMRF-Spring Newsletter Final 15.05.17
It is fantastic to see so knowledgeable and enthusiastic young researchers in my research group. This year, the team is multinational with the Irish students mixing with Belgian and Malaysian. All together they are cracking the code of neuroblastoma microenvironment and tumour cells communication through understanding main differences between conventional cancer cell models and tumours.
The big research plan of the entire team consists of more smaller and focused projects to be completed within 10-12 weeks. All projects are unrestricted, they are driven by the intellectual curiosity of these students. This way is full of ups and downs, frustrations and encouragements when techniques do not work or reagents do not come in as expected. Some cancer concepts can also work differently in the given settings. Simple questions are bringing more challenges than expected. But at the end of the road is the best reward – contribution to the conceptual advancement of neuroblastoma microenvironment.

On Saturday – April 9th, the Conor Foley Neuroblastoma Cancer Research Foundation had their annual fundraising Dinner. This year the theme of the Dinner was Jungle Jazz in memory of the favourite movie of Conor – Madagascar at Trim Castle Hotel.
So many people came to support this fantastic family. The family, who lost their beloved son to neuroblastoma, but has found unacceptable to stop their fight against neuroblastoma. They do know that a cure won’t be found tomorrow. Instead, it may take time, money and efforts to crack the code of this disease so other kids can do better. Thier deal with the situation is priceless and infectious – none can stand still around.
If you asked me after completion of my PhD, would I have ever thought of further education? I would have said – unlikely. Maybe short-term courses to advance my skills, but definitely no to a different field and a 2 years commitment.
Never say never. About four years ago, I started to feel uncomfortable with where I was – a piece of my life jigsaw was missing… I looked up different courses for further education in my field and for anything just relevant to my day job, like project management or teaching. I was even looking around for another job. But nothing…Nothing could be compared with my long life affair – science. This is the only thing that fuels me regardless the career or grant success trajectory.
Ten years after PhD I decided to do Masters in Science Communication, but part-time. The full-time job, family and research challenges did not leave me a choice. This was the same missing piece of the jigsaw. There were a lot to learn exploring another dimension – social sciences. All concepts and ideas of social sciences were studied through lenses of my current interests: cancer research, gender issues, science for public to name the least.
The experience was priceless. It is also inspired me to look outside the ‘box’, see research everywhere and communicate it, and last but not least to start my own blog.

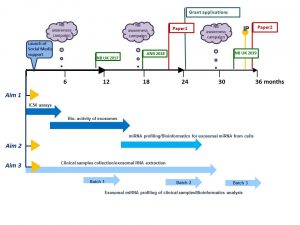
A Research Project Grant funded by National Children’s Research Centre will be starting in April.
The ultimate aim is to identify biomarkers of tumour response to drugs in the blood of children with high-risk neuroblastoma.
Challenge: Treatment regimens for patients with high-risk neuroblastoma involve intensive, multi-modal chemotherapy. Many patients response to initial therapy very well, but has only short-term effects, with most becoming resistant to treatment and developing progressive disease.
The project has two parts which complement each other.
Part 1
Part 2
How does this project contribute to the biomedical community?
This study aims to contribute to the better understanding of the disease mechanisms and scientific knowledge in the area, and in particular how neuroblastoma cells communicate with other cells helping tumour to create a unique microenvironment and protect themselves from chemotherapy pressure. The new data will give insights in biologically active proteins and miRNAs involved in cell-to-cell communication and drug responsiveness.
What are potential benefits of the proposed research to neuroblastoma patients?
This project aims to develop exosomal biomarkers of tumour response to drugs that might be used to help select patients for treatment and identify novel targets for the development of more effective personalised therapy with the anticipated improvement in outcomes. This work will contribute to the more efficient design of re-initiation treatment, sparing patients unnecessary rounds of chemotherapy and ultimately increasing survival. These new circulating markers will benefit children with high-risk neuroblastoma whose tumours are relapsed leading to less harmful and more tailored treatment options and improving their quality of life.
There is no short answer. Research is a slow, meticulous process of testing theories and finding out which ones work.It is exactly the same for both curiosity- and disease- driven questions. Long years of ground research full of ups and downs are critical for any breakthrough or progress. Very often with more downs than ups. Importantly, all researchers build on the work of their predecessors. This is the nature of science.
To understand the world around us, we have to do be curious and do “blue sky or curiosity-driven” research. It is a long shot, but this type of research can lead to practical applications down the road. One of the most recent examples is a drug Vismodegib (Erivedse) to treat basal cell carcinoma (the most common type of skin cancer) approved by the FDA in 2012. This drug targets genes of a hedgehog-associated signalling pathway. Defects in this pathway were found to drive many cases of skin cancer. But, how this relationship was found? Blue sky research!
Researchers studied hedgehog signalling in fruit flies and mice. One of the researchers had a strong interest in a fruit fly gene called hedgehog. If this gene is defective, then fly embryos look stubby and hairy aka a hedgehog. Further research brought more interesting facts and relationships leading to the identification of a drug that can stop the function of this faulty gene. Decades later with the advancement of genome sequencing, the defect in hedgehog signalling pathway genes was identified in patients with locally advanced and metastatic basal cell carcinoma.
What would happen if there were no research in fruit flies and mice? There would have been no rationale to create a drug like Vismodegib!
The best discovery research is unrestricted. It is driven by intellectual curiosity and conceptual advancement. More such curiosity- driven research is needed. For every medical breakthrough, for every Vismodegib, there were hundreds of blind alleys and failed ideas.
The research is a long-term investment. This contradicts to the short-term life of the politicians and governments who give the money. They do not take the risks. So, the discovery research becomes critically underfunded.
Fundraising creates opportunities for blue sky research and developing cancer treatments.
Thank you all who support cancer research charities!
This week Newpark Hotel Kilkenny is hosting the Irish Association for Cancer Research annual meeting 2017.  This meeting is the biggest event for Irish cancer researchers.
This meeting is the biggest event for Irish cancer researchers.
This is the first time in the history of the IACR meetings when an entire plenary session is solely dedicated to challenges and advancements in childhood cancer.
This session will unite Internationally recognised leaders in childhood cancer research. They will speak about what we know about origin and evolution of childhood cancers (Prof. Tariq Enver), how blood biomarkers can help in stratification and treatment of children (Prof. Sue Burchill), what impact Down syndrome has in the white blood cell cancer development and progression (Prof. Irene Roberts), how epigenetic changes affect tumour pathogenesis and future of therapeutics targeting theses changes (Prof Raymond Stallings).
Today, we are celebrating International Childhood Cancer Day to raise awareness and to express support for children and adolescents with cancer, survivors and their families.
Childhood cancer is an umbrella term for a great variety of malignancies which vary by site of disease origin, tissue type, race, sex, and age.
The cause of childhood cancers is believed to be due to faulty genes in embryonic cells that happen before birth and develop later. In contrast to many adult’s cancers, there is no evidence that links lifestyle or environmental risk factors to the development of childhood cancer.
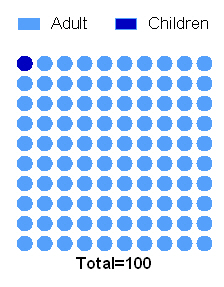
Every 100th patient diagnosed with cancer is a child.
In the last 40 years the survival of children with most types of cancer has radically improved owing to the advances in diagnosis, treatment, and supportive care. Now, more than 80% of children with cancer in the same age gap survive at least 5 years when compared to 50% of children with cancer survived in 1970s-80s.
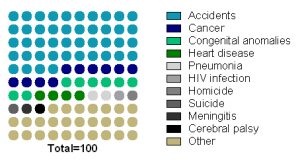
Childhood cancer is the second most common cause of death among children between the ages of 1 and 14 years after accidents.
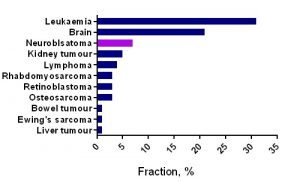
Unfortunately, no progress has been made in survival of children with tumours that have the worst prognosis (brain tumours, neuroblastoma and sarcomas, cancers developing in certain age groups and/or located within certain sites in the body), along with acute myeloid leukaemia (blood cancer). Children with a rare brain cancer – diffuse intrinsic pontine glioma survive less than 1 year from diagnosis. Children with soft tissue tumours have 5-year survival rates ranging from 64% (rhabdomyosarcoma) to 72% (Ewing sarcoma).
For majority of children who do survive cancer, the battle is never over. Over 60% of long‐term childhood cancer survivors have a chronic illness as a consequence of the treatment; over 25% have a severe or life‐ threatening illness.
References:
Gatta G, Botta L, Rossi S, Aareleid T, Bielska-Lasota M, Clavel J, et al. Childhood cancer survival in Europe 1999-2007: Results of EUROCARE-5-a population-based study. Lancet Oncol. 2014.
Howlader N, Noone A, Krapcho M, Garshell J, Miller D, Altekruse S, et al. SEER Cancer Statistics Review, 1975-2011. National Cancer Institute.
Lackner H, Benesch M, Schagerl S, Kerbl R, Schwinger W, Urban C. Prospective evaluation of late effects after childhood cancer therapy with a follow-up over 9 years. Eur J Pediatr. 2000.
Ries L a. G, Smith M a., Gurney JG, Linet M, Tamra T, Young JL, et al. Cancer incidence and survival among children and adolescents: United States SEER Program 1975-1995. NIH Pub No 99-4649. 1999;179 pp
Ward E, Desantis C, Robbins A, Kohler B, Jemal A. Childhood and Adolescent Cancer Statistics , 2014. CA: Cancer J Clin. 2014.
This week can be rated for sure as feeling good, excited and accomplished. A UK based charity – Neuroblastoma UK has awarded a small grant to characterise a pre-clinical model of neuroblastoma which is a collaborative project between our lab and Tissue Engineering Research Group at RCSI. This project will study features of neuroblastoma cells growing on collagen-based scaffolds. The NBUK grant will contribute to one of the most expensive parts of the study – characterisation of cell secreting proteins using antibody-based profiling platforms.

Another research was accomplished yesterday – John Nolan had his Voice Viva examination and successfully defended his PhD Thesis. This 3 year PhD project was funded by the National Children’s Research Centre. As his supervisor, I am delighted for him and wish him best of luck in his research career.
