Neuroblastoma is a childhood cancer. The word neuroblastoma consists of two words neuro and blastoma.The term neuro refers to nerves, blastoma – to a cancer of immature cells.
It starts in some types of nerve cells during embryo development.transforming immature nerve cells into cancerous cells. This type of cancer occurs most often in infants and young children mostly under the age of 5 years old.
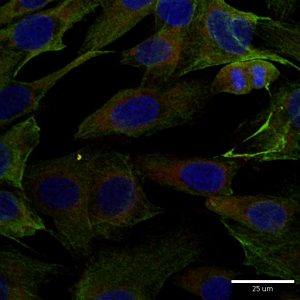
Neuroblastoma cells
Neuroblastomas behave very differently:
Cells can grow and spread quickly,
Cells can grow slowly
Cells can die for no reason, so a tumour goes away on its own.
Cancer is an umbrella term that covers a group of diseases sharing the common features but diseases vary by site of origin, tissue type, race, sex, and age. One of the main features is an uncontrollable growth of cells. These cells are capable of spreading to other parts of the body. This process is also known as invasion and metastasis.
Though cancer in kids is not the same as in adults, childhood cancer cells behave in the same way. They grow uncontrollably and can travel to new destinations in the body.
Mission
To increase the understanding of neuroblastoma pathogenesis,
progression and treatment failure and to improve survival
and quality of life for children with neuroblastoma.
Main Objectives
To consolidate a platform for global collaboration
To establish networks of multidisciplinary caregivers
To develop new trial protocols
To develop standards for radiotherapy and surgery
To develop SOPs for biomaterial collection, handling and storage
To develop SOPs for application of major research technologies
It is always a pleasure to host undergraduate students during summer months. Two students joined the RCSI Research Summer School (RSS) Programme. Both are working on the NCRC funded project to understand mechanisms that drive neuroblastoma pathogenesis. None of them had a prior lab experience, but nothing is impossible under John’s supervision.
A full concentration on every single step of the research.
My PhD student John Nolan together with other 41 candidates graduated at the RCSI’s 2017 June Conferring ceremony which took place in the College Hall of 123 St. Stephen’s Green.
He continues his research in neuroblastoma as a Postdoctoral researcher on the project funded by the National Children’s Research Centre. I am glad to be able to keep expertise and young talents in our team.
The research is a long-term investment. It is always built up on the work of the predecessors. Keep research running is crucial to make the dreams come true. Dreams for better treatment options and quality of life.
Thank you to everyone involved in raising funds for CMRF!
It is fantastic to see so knowledgeable and enthusiastic young researchers in my research group. This year, the team is multinational with the Irish students mixing with Belgian and Malaysian. All together they are cracking the code of neuroblastoma microenvironment and tumour cells communication through understanding main differences between conventional cancer cell models and tumours.
The big research plan of the entire team consists of more smaller and focused projects to be completed within 10-12 weeks. All projects are unrestricted, they are driven by the intellectual curiosity of these students. This way is full of ups and downs, frustrations and encouragements when techniques do not work or reagents do not come in as expected. Some cancer concepts can also work differently in the given settings. Simple questions are bringing more challenges than expected. But at the end of the road is the best reward – contribution to the conceptual advancement of neuroblastoma microenvironment.
The Neuroblastoma Research Dream Team 2017: Dr. John Nolan, NCRC funded researcher, RCSI, Joe O’Brien, TCD MSc student, Ciara Gallagher, DIT undergraduate student, Jessica Tate, RCSI Medical student, Larissa Deneweth, Erasmus student, Ghent, Ying Jie Tan, TCD MSc student.
The ultimate aim is to identify biomarkers of tumour response to drugs in the blood of children with high-risk neuroblastoma.
Challenge: Treatment regimens for patients with high-risk neuroblastoma involve intensive, multi-modal chemotherapy. Many patients response to initial therapy very well, but has only short-term effects, with most becoming resistant to treatment and developing progressive disease.
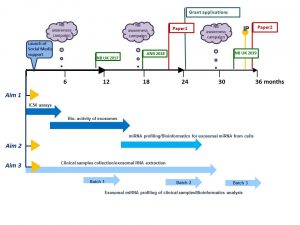
The project has two parts which complement each other.
Part 1
We will study cell-to-cell communication using cell-based models. We will collect exosomes, small envelopes containing bioactive molecules, produced by drug-resistant cell lines to treat non-cancerous cells. We will measure the effect of exosomes on non-cancerous cells by counting cell growth, examining their shape and metabolism. We will also examine whether non-cancerous cells treated with exosomes become less responsive to chemo drugs.
We will treat neuroblastoma cells with a drug and collect exosomes before and after treatment. We will profile exosomes to identify any changes in their miRNA content. MiRNA are very small pieces of genetic material that can change the way cell feels and works. This step will help to find biologically active miRNA that can trigger cell resistance to drugs. These biologically active miRNA can represent biomarkers of tumour response to chemotherapy.
Part 2
We will screen clinical samples for exosomal miRNA in response to drug treatment. We are planning to use a small sample of blood taken from neuroblastoma patients during routine examinations before, during and after chemotherapy.This step will help to find clinically relevant miRNA of tumour responsiveness to chemo drugs.
The plans for 3 years
How does this project contribute to the biomedical community?
This study aims to contribute to the better understanding of the disease mechanisms and scientific knowledge in the area, and in particular how neuroblastoma cells communicate with other cells helping tumour to create a unique microenvironment and protect themselves from chemotherapy pressure. The new data will give insights in biologically active proteins and miRNAs involved in cell-to-cell communication and drug responsiveness.
What are potential benefits of the proposed research to neuroblastoma patients?
This project aims to develop exosomal biomarkers of tumour response to drugs that might be used to help select patients for treatment and identify novel targets for the development of more effective personalised therapy with the anticipated improvement in outcomes. This work will contribute to the more efficient design of re-initiation treatment, sparing patients unnecessary rounds of chemotherapy and ultimately increasing survival. These new circulating markers will benefit children with high-risk neuroblastoma whose tumours are relapsed leading to less harmful and more tailored treatment options and improving their quality of life.
This is the first time in the history of the IACR meetings when an entire plenary session is solely dedicated to challenges and advancements in childhood cancer.
This session will unite Internationally recognised leaders in childhood cancer research. They will speak about what we know about origin and evolution of childhood cancers (Prof. Tariq Enver), how blood biomarkers can help in stratification and treatment of children (Prof. Sue Burchill), what impact Down syndrome has in the white blood cell cancer development and progression (Prof. Irene Roberts), how epigenetic changes affect tumour pathogenesis and future of therapeutics targeting theses changes (Prof Raymond Stallings).









 This meeting is the biggest event for Irish cancer researchers.
This meeting is the biggest event for Irish cancer researchers.