The new norm, new challenges, new excitement and new achievements! We all proud to say that we completed 10K Vhi Womens Mini marathon socially distanced. Our paces were so different that distancing came absolutely natural. We ran it individually but were a team mentally. Even the capricious Irish weather was our ally. The Sun was bright. The air was fresh and crispy.
This was an individual challenge #POWEROF10: just you and the trail. 10 laps around St Stephen’s Green park were to make the target 10K in aid of Childhood Cancer Awareness Month. The celebration of life, therapeutical advancements, the strength of little patients battling their cancer and their families, doctors and carers who are supporting them in their journey. The emphasis on the gaps in available treatments and diagnosis and the importance of research that needs funding.
Personally, my 10K were split into two parts. The first 4K were full of arguments with my body. Why didn’t I like to do laps? Could I complete 10K? Was I fit to do it? Keep going! No walking – better slow jogging. Did one lap make 1K? Should I do a longer lap instead? And so on and so forth. Then, the second part kicked in. My body stopped arguing and began to enjoy it. I noticed beautiful Autumn colours on the trees, people walking around with a cup of coffee or chatting away, saw my team members overtaking me, and our volunteers counting our laps. People on the street and in the park were cheering us up. What a wonderful and fulfilling day!
As Catherine says: “The 10 Laps 10km challenge was tough! Like many people, I took up running casually during the lockdown, however, I never did more than a couple of kilometres at once, so I was absolutely not prepared for running 10. But the cheers from our socially distanced spectators and all the online support we received meant I got through it. Also knowing what a positive impact this challenge could have for the future of childhood cancer treatment provided plenty of motivation to finish the race 💛🎗”
10K by 6 team members socially distanced. #POWEROF10. Go Gold! Let’s reach 1.5k in donations!
Our Go Fund Me page is still open until this Sunday (October 11th midnight) if you wish to support us.
Our team is expanding – we are welcome our new PhD student Ellen King!Her project will add another dimension to neuroblastoma research. She will look into potential targets on the surface of neuroblastoma cells resistant to therapy and investigate how we can strengthen the patient immune systemresponse.
Like everyone, my current workspace looks very different from what it normally looks like. I have just joined the Cancer Bioengineering Group as a PhD student in the midst of the pandemic. Certain moments like induction day or meeting my new lab mates, will all be done virtually due to the pandemic. Luckily, I have spent the last year working as a research assistant at RCSI and this has taken away all the stresses of finding my way around a new campus and indeed making friends. Without a doubt, the transition is and will be a strange one but the excitement and enthusiasm haven’t gone anywhere!
Recently, my days as a researcher have been spent at my lovely, newly-built (with the help of IKEA instructions) home desk. And as the picture I have standing proudly beside my laptop says, there really is no place like home. I feel very lucky to be able to safely work from home and continue my research while so many people are now without jobs or are risking their lives to keep people safe during the pandemic.
“NÍL AON TINTEÁN MAR DO THINTEÁN FÉIN” – THERE IS NO FIRESIDE LIKE YOUR OWN
Most days I wake up early and go for a run along the lovely canal beside my house. This is a great way to wake up my brain and is also great preparation for our virtual VHI mini-marathon on the 7th of October 2020 in honour of Childhood Cancer Awareness Month. I start work at around 9am, which at the moment is mostly research, reading papers and writing a literature review in preparation for my return to the lab soon. I miss the experimental side of my research and am really excited to start this new exciting project.
Today marks the start of Childhood Cancer Awareness Month.
Three girls fountain in Mainz Germany
I like this photo of a lovely fountain capturing 3 girls under umbrellas (Drei-Mädchen-Brunnen) in Ballplatz Mainz. It is about a happy childhood; every child deserves a happy childhood. So, I select it again to support #ChildhoodCancerAwarnessMonth.
Childhood cancer is an umbrella term for many other types of this disease. This month is a big channel to support and learn more about kids with cancer, their loving families, the doctors and caregivers who looking after them and treating them, the young survivors of cancer and those kids and teens who lost their battle, and the scientists who working hard to find a way to stop childhood cancer.
When it comes to a disease, we have to acknowledge that children are not little adults. They are constantly developing. So their diseases have a different way to progress and respond to treatment. This is very true for childhood cancers. For example, children diagnosed with neuroblastoma before a 1.5 years old mark will do better than older children.
Every 100th cancer patient is a child. Cancer is the 2nd most common cause of death among children after accidents. The most common types of childhood cancer are:
Leukaemia and lymphoma (blood cancers)
Brain and other central nervous system tumours
Muscle cancer (rhabdomyosarcoma)
Kidney cancer (Wilms tumour)
Neuroblastoma (tumour of the non-central nervous system)
Bone cancer (osteosarcoma)
Testicular and ovarian tumours (gonadal germ cell tumours)
Now, when my team has expanded, it is so easy to come up with fundraising ideas and then develop one in a well-rounded event. In February, we ran Hot Chocolate Morning to raise awareness in childhood cancer and celebrate the International Childhood Cancer Awareness Day. We have an entire month of September to make this disease visible. It was the first time for some of my team members.
“Last Friday, I got to take part in my first fundraising event at the Royal College of Surgeons in Ireland. Our team hosted a waffle morning for #childhoodcancerawarenessmonth and we are delighted to have raised €403.85 thanks to everyone’s generous donations! Our fundraising does not stop here, in just a few weeks time all 7 of us will be taking on the 8km Hell and Back challenge to raise more awareness and funds for our four chosen charities: CMRF Crumlin, Neuroblastoma UK, and the Conor Foley Neuroblastoma Cancer Research Foundation. We hope everyone enjoyed their little Friday treat!” Catherine Murphy, PhD student funded by Neuroblastoma UK
Here, we are – the Irish neuroblastoma research team landed at the 5th Neuroblastoma Research Symposium in Cambridge. Four poster presentations by four enthusiastic scientists. The two days crash course in neuroblastoma – vibrant, intense, informative.
I had one of the most enjoyable poster sessions in the last few years! A genuine interest in our 3D in vitro cancer models by both academics and Industry. Hope, to keep the ball rolling and strengthen these new links.
The Symposium programme was an excellent balance of the new transnational outcomes with hardcore developmental cellular programmes. From ‘How neuronal precursors select their fate and how they can escape the developmental constraints? How this knowledge can help to advance our understanding of neuroblastoma aetiology?’ to ‘New drugs that demonstrated great potency in pre-clinical studies’ via ‘how we can work together more efficiently to progress quicker’
Indeed, the success of the research meeting became possible thanks to the strategic vision and leadership of organisers!
13:00 – 13:10 Introduction – Neuroblastoma UK & CRUK Cambridge Centre
Session 1: Neuroblastoma biology & prognosis
Cancer Research UK Cambridge Centre Neuro-oncology Programme Session
Chair: Kate Wheeler (Oxford Children’s Hospital)
13:10 – 13:40 Sandra Ackermann (Cologne): The genetic basis of favourable outcome and fatal tumour progression in neuroblastoma
13:40 – 14:10 Rogier Versteeg (Amsterdam): The dark side of neuroblastoma
14:10 – 14:40 Katleen de Preter (Ghent): Improved diagnosis and risk stratification of paediatric cancers using liquid biopsies
14:40 – 14:55 Sue Burchill (Leeds): Self-renewing neuroblastoma cells isolated from bone marrow aspirates of children with stage M disease share a mesenchymal expression signature: an NCRI CCL CSG Neuroblastoma Group Study
14:55 – 15:15 Combined discussion
15:15 – 15:45 Tea with Posters
Session 2: Targeted & combination therapy I
Cancer Research UK Cambridge Centre Neuro-oncology Programme Session
Chair: Marie Arsenian Henriksson (Karolinska)
15:45 – 16:15 Frank Westermann (Heidelberg): Novel metabolic dependencies of MYCN-driven neuroblastoma
16:15 – 16:45 Gerard Evan (Cambridge): Is Myc really master of the universe?
16:45 – 17:00 Melinda Halasz (University College Dublin): Anti-Cancer Effects of Diphenyleneiodonium Chloride (DPI) In MYCN-Amplified Neuroblastoma
17:00 – 17:15 Evon Poon (ICR, Sutton): Pharmacological blockade of high-risk MYCN driven neuroblastoma using an orally-bioavailable CDK2/9 inhibitor
17:15 – 17:35 Combined discussion
Downing College – Main Hall.jpg
17:35 – 19:15 Poster viewing & Drinks
19:30 Symposium Dinner at Downing College (map for dinner)
FRIDAY 12TH APRIL 08:30 – 08:50 Coffee & pastries
Session 3: Neural crest & differentiation therapy I
Chair: Margareta Wilhelm (Karolinska)
08:50 – 09:20 Igor Adameyko (Karolinska): Normal development of sympathoadrenal system resolved with lineage tracing and single cell transcriptomics
09:20 – 09:50 Quenten Schwarz (Adelaide): Guiding sympathoadrenal neural crest cells to the adrenal primordia
09:50 – 10:05 Claudia Linker (King’s College London): Notch coordinates cell cycle progression and migratory behaviour leading to collective cell migration
10:05 – 10:20 Combined discussion
10:20 – 10:50 Coffee with Posters
Session 4: Neural crest & differentiation therapy II
Chair: Gareth Evans (York)
10:50 – 11:20 Karen Liu (King’s College London): ALK and GSK3 – shared features of neuroblastoma and neural crest
11:20 – 11:35 Anestis Tsakiridis (Sheffield): Efficient generation of trunk neural crest and sympathetic neurons from human pluripotent stem cells via a neuromesodermal progenitor intermediate
11:35 – 12:05 Anna Philpott (Cambridge): Using developmental mechanisms to drive differentiation of neuroblastoma
12:05 – 12:20 Combined discussion
12:20 – 13:20 Lunch with Posters
Session 5: Targeted & combination therapy II
Chair: Bengt Hallberg (Gothenburg)
Cancer Research UK Cambridge Centre Paediatrics Programme Lecture:
13:20 – 13:50 Sharon Diskin (Philadelphia): A multi-omic surfaceome study identifies DLK1 as a candidate oncoprotein and immunotherapeutic target in neuroblastoma
13:50 – 14:05 Donne Nile (Glasgow): Manipulation of cancer cell metabolism for neuroblastoma combination therapy with targeted radiotherapy
14:05 – 14:35 Suzanne Turner (Cambridge): CRISPR-dCas9 screens to identify resistance mechanisms to ALK in neuroblastoma
14:35 – 14:50 Combined discussion
14:50 – 15:20 Tea with Posters
15:20 – 15:30 Poster prizes
Session 6: Targeted & combination therapy III
Chair: John Lunec (Newcastle)
15:30 – 16:00 Per Kogner (Karolinska): The PPM1D encoded WIP1 phosphatase is an oncogene significant for cancer development and tumour progression and a druggable therapy target in neuroblastoma and medulloblastoma. A hint as to how aggressive childhood cancer manages with wild-type p53
16:00 – 16:15 Deb Tweddle (Newcastle): Preclinical assessment of MDM2/p53, ALK and MEK inhibitor combinations in neuroblastoma
16:15 – 16:30 Sally George (ICR, Sutton): A CRISPR-Cas9 genomic editing and compound screening approach identifies therapeutic vulnerabilities in the DNA damage response for the treatment of ATRX mutant neuroblastoma
16:30 – 16:45 Miriam Rosenberg (Jerusalem): Expression- and immune-profiling of neuroblastoma-associated Opsoclonus Myoclonus Ataxia Syndrome (OMAS) to identify features of auto- and tumour-immunity
An interesting idea or research question is always motivational. But it is a sketch till you get means to answer them. We, scientists, have to shape them into a proposal showing that we know limitations and have plans B & C if things go differently to planned. Then we apply for funding here and there… and many many times. The number of rejections makes us stronger – I hope. But one day, the idea may hit it right. So, it has happened to me recently and this SFI Award brings so needed fuel to study neuroblastoma.
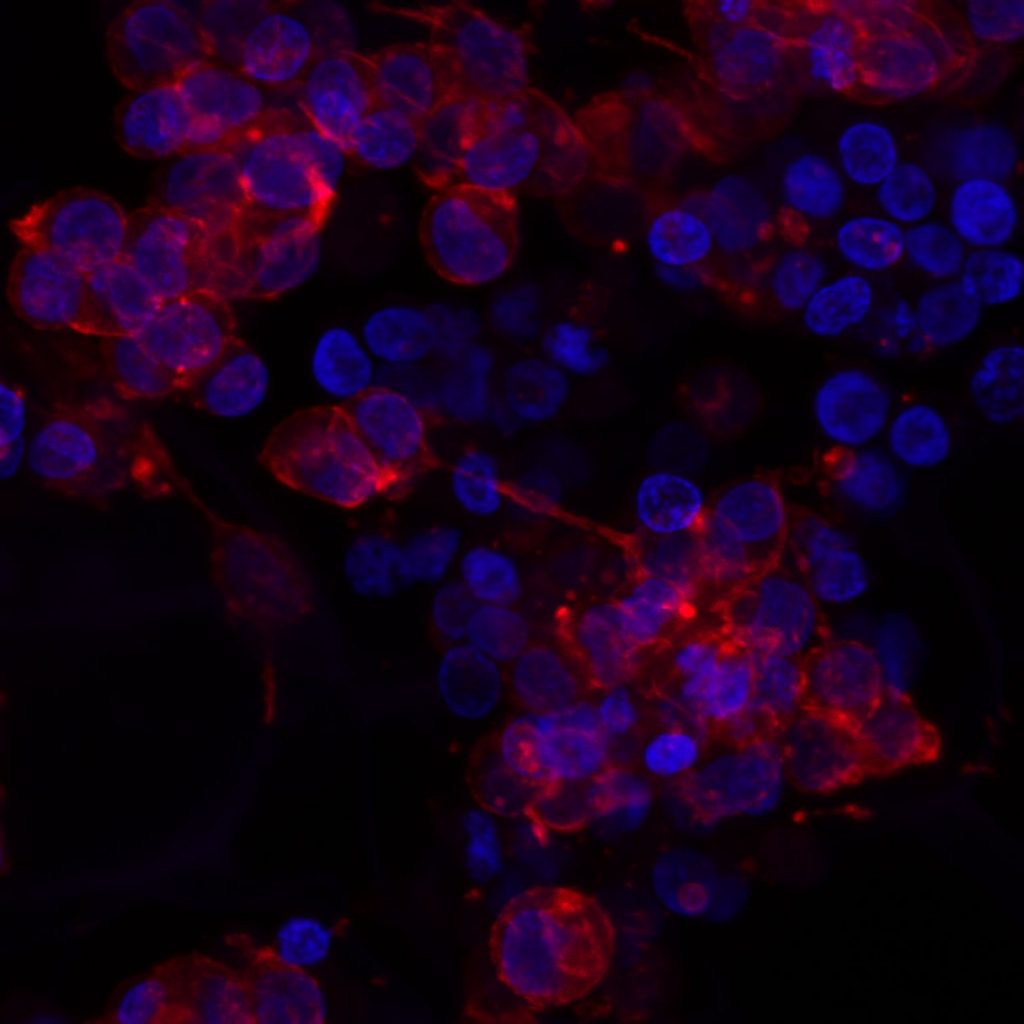
The development and approval of new oncology drugs are very slow processes. This is mainly due to the big differences in the physiology of cancer cells grown on plastic and in the native microenvironment. Tissue engineering of tumour systems has a great potential to bridge this gap. This Award will help to advance our 3D tissue-engineered of neuroblastoma, that can be used in testing new drugs and new combinations of existing drugs.
Neuroblastoma cells grown in 3D
In particular, we will adapt the 3D model to screen different immunotherapies. This treatment option is very attractive both for adults and children because of its specificity and reduced side effects compared to chemotherapy, the current standard of care.
This Award will help my team to get a better understanding how neuroblastoma cells interact with the body environment, particularly with the immune system and how we can use the knowledge to develop new treatments and improve the patient outlook.
Last year I have selected this photo of a lovely fountain capturing 3 girls under umbrellas (Drei-Mädchen-Brunnen) in Ballplatz Mainz in support of #ChildhoodCancerAwarnessMonth. This fountain was built between two Catholic girl’s schools symbolising the separate education and a happy childhood. It is charming on its own. And I’ve select it again.
Every child deserves a happy childhood. Raising awareness about childhood cancer we help to make the dreams of children with cancer come true. Dreams for a happy childhood, better treatment, better quality of life full of love ahead through better funding of childhood cancer research and access to innovative treatments.
Today marks the start of Childhood Cancer Awareness Month.
Three girls fountain in Mainz Germany
The cause of childhood cancers is believed to be due to faulty genes in stem cells that give rise to nerves, skin, blood and other body tissues. For some unknown reasons, the faulty genes can sit quiet and show their ‘bad’ character after birth and programme the cells into cancer cells.
So, there is no evidence that links lifestyle or environmental risk factors to the development of childhood cancer, which is opposite to many adult’s cancers.
Every 100th cancer patient is a child. Cancer is the 2nd most common cause of death among children after accidents.
Children are not little adults and so their cancer. Some childhood cancers have a good outlook and successful protocol of treatments. However, some of the cancers do not respond to the known drugs, or if respond cancer cells find the way to develop resistance and come back being more aggressive. Among theme are some forms of brain tumours, neuroblastoma and sarcomas; cancers developing in certain age groups and/or located within certain sites in the body, along with acute myeloid leukaemia (blood cancer). Children with a rare brain cancer – diffuse intrinsic pontine glioma survive less than 1 year from diagnosis. Children with soft tissue tumours have 5-year survival rates ranging from 64% (rhabdomyosarcoma) to 72%(Ewing sarcoma). Less than50% of children with the aggressive form of neuroblastoma will live beyond 5 years with current treatment strategies.
For majority of children who do survive cancer, the battle is never over. Over 60% of long‐term childhood cancer survivors have a chronic illness as a consequence of the treatment; over 25% have a severe or life-threatening illness.
The most common types of childhood cancer are:
Leukaemia and lymphoma (blood cancers)
Brain and other central nervous system tumours
Muscle cancer (rhabdomyosarcoma)
Kidney cancer (Wilms tumour)
Neuroblastoma (tumour of the non-central nervous system)
Bone cancer (osteosarcoma)
Testicular and ovarian tumours (gonadal germ cell tumours)
On November 20th, the Irish neuroblastoma researchers have met for the first time to set up a collaborative research hub. The aim is to consolidate their expertise and skills in order to crack the neuroblastoma code together.
They all have different science background spanning from molecular and cellular biologists, immunologists, tissue-engineering, bioinformatics, mathematical modelling and clinicians representing RCSI, UCD, TCD, OLCHC and NCRC. During this meeting, researchers talked about their challenges and progress finding out that we are complementing each other projects. Clinicians from different OLCHC departments exposed basic researchers to realities of the disease. None would find this information in academic papers: it is what you see in the clinic and how it works in practice.
Big thank you to Dr Cormac Owens for the invitation and linking us together and Prof Jacinta Kelly for mapping the support available from the NCRC and CMRF.
Our next meeting will be held in RCSI in January 2018.
Happy Birthday the Irish Neuroblastoma Research Consortium!
We hear great news from the US labs that a new treatment is on the way for children with cancer. Most of their research is funded by charities and success stories appear because of the people who want to make dreams come true for kids with cancer and their families. Dreams for longer and healthier life.
Interestingly, the study led by Professor Bernie Hannigan, the University of Ulster, which was published by Medical Research Charities Group, identified main gaps that keep Ireland at the bay:
Childhood cancer research areas are not prioritised, including neuroblastoma.
No Government funding support for childhood cancer research. The research has to compete on general terms with well-funded research groups/centres/clusters focused on the adult cancers (breast, prostate, etc)
No systematic involvement in research of Patients or other lay people.
No medical research charities to fill the gap in childhood cancer research funding.