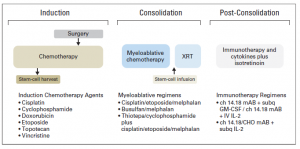
Children with high-risk neuroblastoma is the most challenging group to treat. Current treatment strategy for this group consists of 3 treatment blocks:
- induction: chemotherapy and primary tumour resection;
- consolidation: high-dose chemotherapy with autologous stem-cell rescue and external-beam radiotherapy [XRT];
- post-consolidation: anti–ganglioside 2 immunotherapy with cytokines and cis-retinoic acid.
Up to 50% of children that do respond experience disease recurrence with tumour resistant to multiple drugs and more aggressive behaviour that all too frequently results in death.
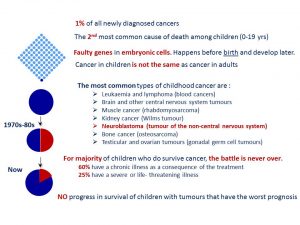
For the majority of children who do survive cancer, the battle is never over. Over 60% of long‐term childhood cancer survivors have a chronic illness as a consequence of the treatment; over 25% have a severe or life‐ threatening illness.
Reference:
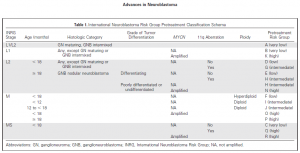
Pinto NR, Applebaum MA, Volchenboum SL, Matthay KK, London WB, Ambros PF, Nakagawara A, Berthold F, Schleiermacher G, Park JR, Valteau-Couanet D, Pearson AD, Cohn SL. Advances in Risk Classification and Treatment Strategies for Neuroblastoma.J Clin Oncol. 2015 Sep 20;33(27):3008-17.