Ok. Now, when the stress of the presentation is over, I am happy to share new technologies used during the SIOP2016. As I mentioned yesterday, my work was selected for e-poster presentation. It looked this way:
This is e-poster station, where anyone can look up all posters displayed during the meeting.
It is definitely a step forward. Anyone can look up any poster, listen to a commentary recorded by the author, zoom in and out and send a request/comment to the author. It looks cool and trendy. Though, you can feel invisible as no physical copy displayed in a designated area. No crowds of poster presenters and judges. No waiting faces desperate to share their study…
The actual Poster Discussion session was a traditional presentation when my poster was up on the big screen, I had 8 minutes to convince the audience navigating through figures. This session was late and no many attendees survived to come and challenge your statements. Nevertheless, it was enjoyable experience. 🙂
SIOP is the International Society of Paediatric Oncology. It is a global multidisciplinary society representing doctors, nurses, other health care professionals, scientists and patients or their relatives. The Society’s motto is ‘no child should die of cancer’. The meeting 2017 is being held in Dublin, the city where I live and work.
Indeed, it was appealing to attend the key meeting in childhood oncology field. As any participant, I had an opportunity to submit an abstract about my research. To no surprise at all, I received email notifying me on my work being selected for e-Poster presentation. Common stuff. The email also said that it would be displayed at designated stations, like big screens throughout the meeting. Very unusual format, but we are living in the digital technology era; things are changing all the time. So, I would not need to stay by the poster this time. Great – more time for networking and talks.
Then I received another email informing about a Poster Discussion session, which I assumed to be a standard procedure when a group of selected piers stand by your poster and ask Qs. None comes in majority cases. A participant stands and waits and waits till the session is over. So, of course I took it easy.
A day before the meeting, I downloaded the meeting app and started to browse along the content and features. Out of curiosity, I checked details of the Poster Discussion session. This was the moment of mental breakdown – I discovered being selected for an oral poster presentation! My chances were 1 in 1475 (the number of submitted abstracts). I should probably also buy a lottery ticket tonight. Could lucky things come together?
I will reflect on the new e-poster presentation experience later today…
We do not hear much on neuroblastoma or childhood cancer in our everyday life unless we know a child affected by the disease. How much information can we get from newspapers? How do newspapers report it? What is their focus – a child, his/her family or social circles? In the next posts I will try to get insights from the content of newspaper’s stories.
To start with, I needed to select those newspaper articles that cover a story of a child with cancer over a period of time. To do that I selected a recent period from January 1, 2010 to December 31, 2015 because two major events happened during this time.
The first was the 2011 Pulitzer Prize book written by Siddhartha Mukherjee ‘The Emperor of All Maladies: A Biography of Cancer’ which describing the history of both adult and childhood cancer treatment development and research (Mukherjee 2010). Importantly, this book inspired to produce a documentary film of three episodes of two hours each and released in 2015 (Goodman 2015). Researchers in social sciences agree that the publication of a prominent popular science book can lead to increased media interest in the issues raised in the book (e.g. (Nisbet & Fahy 2013).
Another most recent milestone was a breakthrough in childhood cancer management – the FDA approval of a novel drug Unituxin (dinutuximab) for neuroblastoma, the most common solid tumour in children (U.S. Food and Drug Administration 2015).
The timeline of media coverage analysis
next step is actual paper selection. There is an archive of all newspapers and magazines called Nexis®UK database. This database stores copies of all printed papers and magazines worldwide as well as online versions.
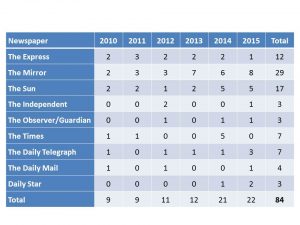
Then an a search for articles carried out looking for key words:‘child’, ‘children’, ‘childhood’, ‘kid(s)’, ‘cancer (s)’, ‘tumour (s)’, ‘treatment’, ‘chemotherapy’, ‘radiation’ and their combinations. Only articles published by the UK national newspapers and included key words in either the headline or text were selected. The search returned 255 articles. Of 255 articles, 84 contained a story about a child with cancer. The rest were standardised obituaries in the ‘announcements’ or ‘deaths’ sections, horoscopes containing the word ‘cancer’, fundraising and charity activities not involving an identified child, funding initiatives related to pure cancer research and service, reports on scientific achievements or challenges were excluded.
The selected 84 articles were published by the broad range of local and national papers that are daily on sale through news outlets to a general public in the UK.
Summary of selected newspapers
The Q1: What has been the level of media attention to childhood cancer?
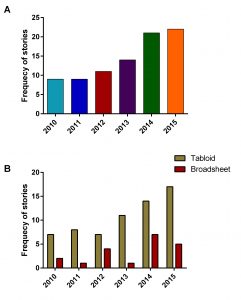
In the last three years, in average 20 articles per year across 9 UK newspapers were published telling us a story about a child with cancer. In other terms it is less than 2 stories per month. It is not enough to raise awareness, educate the public and form their opinion. Tabloid editorial was more interested in this type of stories than broadsheet. This observation is likely due to the nature of tabloid paper interests looking for people personal stories, entertainment, sports and scandal.
Unfortunately, no change in media coverage of childhood cancer was observed around these two milestones (in 2011 and 2015). All together it suggests that neither of them had a strong influence on journalists or editorials regarding childhood cancer coverage.
Frequency of stories about a child with cancer by year (A) and type of newspaper(B)
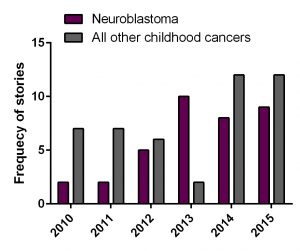
Interestingly, the growing trend in media coverage of children with cancer occurred by the increase in neuroblastoma coverage. Neuroblastoma had a nearly two fold boost in 2013 vs 2012 and then slightly declined in 2014 and 2015. Nevertheless, the FDA approval did not trigger attention to this cancer.
Frequency of stories about a child with cancer by cancer type
The conference on models and tumour microenvironment has brought together International experts in this field. Two keynote speakers (Peter Friedl, Radboud UMC/MD Anderson and Andrew Ewald, John Hopkins University) presented exhaustive experimental data on plasticity and microenvironmental control of cancer invasion and metastasis.
Their research teams independently found that
Tumour cells migrate collectively as a team from a piece of tumour like a group of people who changed their minds and decided to travel by bus when the majority stayed camping. However, Andrew Ewald acknowledged that they are not pioneers in this discovery. In 1976 Liotta observed migration of tumour cells in a group of 6-10 cells.
A migration group of cells has their leaders who crave the path through surroundings to the new locations.
Leader cells depend on cancer types. It can be any tumour cell in some cancer types or a specialised one.
Migrating cells take shape and follow the pattern of tissues to be invaded.
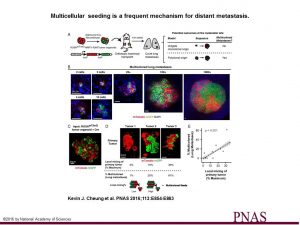
The experiments by Ewald’s research team on collective cell migration. In short, they co-implanted two lung tumour cell populations labelled differently into mice. One cell population had a green protein tag, another had red. After 6-8 weeks, researchers examined metastases and found that they had a mixed population of green and red tumour cells.
Multicellular seeding is a frequent mechanism for distant metastasis. (A) Schema of multicolor lineage tracing assay. ROSAmT/mG;MMTV-PyMT tumor organoids were treated with adenoviral Cre to induce recombination from membrane tdTomato (mTomato) to membrane eGFP (mGFP). Mosaic tumor organoids were then transplanted into nonfluorescent NSG host mice. After 6–8 wk, lungs of these mice were harvested. If metastases arise exclusively from single-cell seeding, there should be only single color metastases. In contrast, multicellular seeding should produce metastases with both colors. (B) Representative micrographs of polyclonal lung metastases of different sizes. n = 355 polyclonal metastases, across 16 mice and 4 independent experiments. (C) Representative micrograph of a mosaic tumor organoid treated with adeno-Cre and grown in 3D Matrigel with intermixing of red and green tumor cell clones. (D and E) Representative micrographs of primary tumors arising from mosaic tumor organoids transplanted into NSG host mice. Primary tumors varied in their local mixing of red and green tumor cell clones (local mixing %). These differences correlated with the percentage of multicolored metastases detected in the lung (% multicolored). n = 12 mice, 4 independent experiments, 4,072 metastases. Correlation determined by Spearman rank test for samples with more than five lung metastases per mouse. (Scale bars, 20 μm in B and C, and 2 mm in D.)