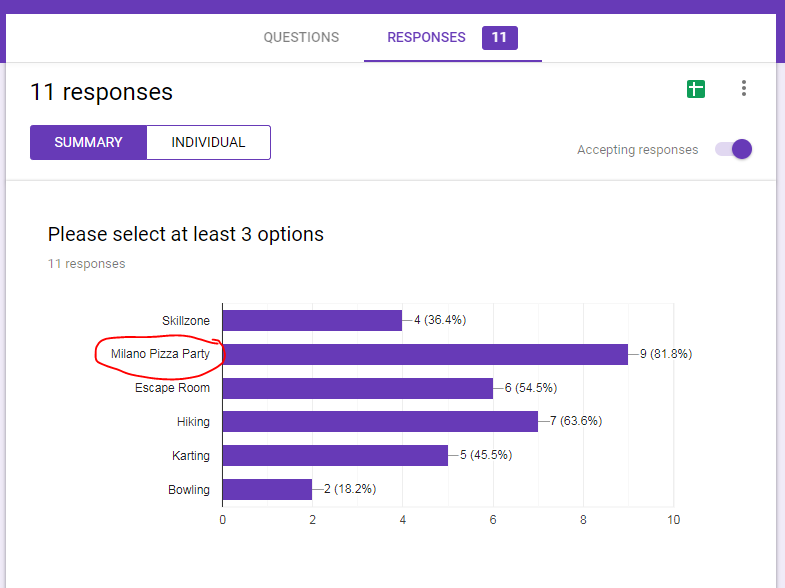
Our team has expanded. Now, we are 11 – a great mix of cultures and science backgrounds! But it comes at a price – how to agree on even simple activities? Shall we go hiking? Bowling? Karting? Room Escape?
Poll it! Vualá

Blog about neuroblastoma research
My WordPress Blog is about neuroblastoma biology and Cancer Bioengineering Group

Our team has expanded. Now, we are 11 – a great mix of cultures and science backgrounds! But it comes at a price – how to agree on even simple activities? Shall we go hiking? Bowling? Karting? Room Escape?
Poll it! Vualá
Across countries and continents, we are celebrating International Childhood Cancer Day (ICCD).We do it to raise awareness tto raise awareness of childhood cancer, its consequences for children and their parents and make it as a priority for Governments and research.
My team research is focused on neuroblastoma biology. This is a solid tumour of undeveloped nerves. Some forms of neuroblastoma spread quickly and become very aggressive and challenging to treat. We are searching for the weaknesses that can be targeted with drugs.

Today, we team up with Amorino to run the Hot Chocolate Morning to raise funds for Childhood cancer research charities – Children’s Medical Research Foundation/National Children’s Research Centre and the Conor Foley Neuroblastoma Cancer Research Foundation. Research advances our knowledge and helps to develop new treatments.

A guessing game was a part of the event. Everyone had a chance to guess how many marshmallows fitted in the cell culture flask T75. The guesses ranged from as low as 95 to as high as 500. Fortunately, one of the participants gave an absolutely correct answer. Micheal Flood put on 173 and won. Her fantastic ability to guess is incredible! Congratulations!!! Well done to all!
We raised 698.91 Euros for childhood cancer research! We thank everyone who came along and supported the Hot Chocolate Morning & the International Childhood Cancer Day 2019!
Many special thanks go to Amorino for delicious Italian hot chocolate & tasty bites contributors!

International Childhood Cancer Day (ICCD) was founded in 2002 by Childhood Cancer International (CCI). Each year on February 15th we unite together to recognise childhood cancer as a national and global child health priority & to raise support, funding and awareness of this devastating
This year we team up with Amorino to run Hot Chocolate Morning. Please come along! All proceeds go to CMRF/NCRC and CFNCRF.
If you can’t join us, you can simply follow the link and donate ‘a cup of coffee/hot chocolate’ to CMRF Crumlin, the Conor Foley Neuroblastoma Research Foundation & Childhood Cancer Foundation
Coming to live and work for a short period ignites opposite feelings. Should I see all the places recommended by Tripadvisor or do it at my pace as it happens? What if I miss something worthy? Perhaps, your own intuition balances somehow both.
I have discovered and loved two buildings in Baltimore. One is the building of Barnes & Noble bookstore in Inner Harbour and the other is Mount Vernon Place Church. Both have a great history behind and give a very warm feeling when you are inside.
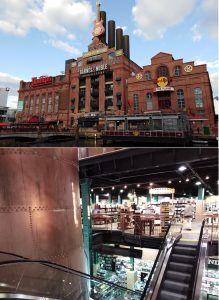 Barnes & Noble bookstore is located in the former Power Plant. The features are easily spotted. From outside, the building looks like a Plant for modern social activities. Ugly slightly, isn’t it? Though, it is a different feeling when you enter the bookstore. The Plant scaffolds, chimneys and pipes are nicely crafted into a warm welcoming environment. Even lights are dimmed as back then. Rambling through the bookshelves and feeling the magic of the place and unread stories on them. You can pick up a book, sit where you are and enjoy the reading. Maybe it is the feeling of my childhood full of books and hours of reading?
Barnes & Noble bookstore is located in the former Power Plant. The features are easily spotted. From outside, the building looks like a Plant for modern social activities. Ugly slightly, isn’t it? Though, it is a different feeling when you enter the bookstore. The Plant scaffolds, chimneys and pipes are nicely crafted into a warm welcoming environment. Even lights are dimmed as back then. Rambling through the bookshelves and feeling the magic of the place and unread stories on them. You can pick up a book, sit where you are and enjoy the reading. Maybe it is the feeling of my childhood full of books and hours of reading?

Mount Vernon Place Church is next to the Washington Monument and recalls old Catholic Cathedrals in a Victorian Gothic Style. Built in 1872, the Church is actually the United Methodist Church from the very beginning. It is beautiful inside as well as outside. The stained glass and carvings have Nature themes. A big rose window in the rear of the church was inspired by the one in Notre Dame. It has an interesting history which you can read here. I discovered this place by chance and am glad that this chance came from my host family. I saw the interior not only the Church but also Asbury House. The mansion was a home to the first bishop of the Methodist Church in America – Francis Asbury (1745-1816). Have a look at the pictures, the furniture is well preserved, the staircase is similar to the one you can see in Slane Castle. Its light design makes it looks flying. Indeed, not everyone could use it at that times. Servants had a plain version at the back of the house, so none could have seen them moving in and out. Lots of blue and carved wood in the rooms. Incredibly beautiful.


What is a must-see in Ireland? Right: visit Guinness brewery at St. James’s Gate and have a pint of right Guinness. It is one of the most recognised and famous beer brands. Rumours say Dublin is the only place where Guinness tastes Guinness. Traditions, traditions and traditions. Though the one we like most Guinness Draught is a relatively new addition – it was introduced almost 200 years after the brewery establishment in 1759 by Arthur Guinness.
So, what if you like tastes ‘outside the box’? Then Guinness brewery in Baltimore is for you. Respecting the Father, they do completely different stuff. Imagine, 16 different tastes, including the one we know! You can have a guided tour of the brewery, hear the great story and do a beer tasting. Have you tried one? Not, the one in the pub or with the friends at BBQ. It is a special way to feel the bouquet of flavours and taste the difference. There is a difference between the beer drunk straight from the bottle and from the glass. Because you can smell it as simple as that.

During our guided tour, we rambled inside the experimental brewery, learn the basics of beer production, tasted 4 types of beer: Guinness Blonde, Oatmeal Pale Ale, Guinness Draught and Guinness Milk Stout. Three were absolutely new for me. I liked Oatmeal Pale Ale, found Milk Stout a bit dessert style, Blonde – too citrusy. Do not forget, another 12 you can taste at the bar in a special set! However, to enjoy the most you have to bring your friends. All is much better with the right company!

Can you control the time? I can’t and know none who can. It flies, when things around you work out, and drags on when not. The time flies for me here in Baltimore. It feels so intense sometimes and then slightly slows down. I take pictures almost of everything: the path’s signposts when rambling in the network of Johns Hopkins Buildings, the first frosty morning, joyful deer at the backyard of my host family house, outdated clothes in the shop…
In the past, I had a similar journey to Ireland. It was 3 months research placement during my PhD. Did I like it – oh, yes I did! I travelled a lot, felt romantic and changed my life on my return home. But I did not run a diary or tag my way on Facebook. I have learnt the lesson: do it even more intense as you can’t travel back in time and write down your experience. It may be funny or educational to read in a couple of years! I become addicted to it though not always have time to do it.
I like the people who I am working with. They are a fantastic bunch of self-motivators and open-minded personalities. They are workaholics either naturally like me or because of the exciting projects they do like I do. Who knows, but very likely because of both. Isn’t it a dream to have an exciting project and great people around you? The luck like this gives you wings.

The host family – is my other great luck! This luck was crafted as a parallel story when none knew how the Fulbright application and an American enthusiast learning Russian may intersect. You would not believe, but parallel lines can be non-parallel sometimes! His journey to my home city in Russia paved the way to the opportunity to stay at his aunt’s house.
Every day 50 min drive to and from Hopkins opens up the other side of the local lifestyle and infrastructure. What are the rush hours? How many drivers are signalling before taking a turn? How do they call the shopping trolley? How parking system works?
Experiencing life as an American working in Baltimore.
This is how my journey began. On Tuesday, I received an invite from the Children’s Medical Research Foundation to attend the Annual Summer Gala Dinner at the Water Club in Manhattan on Thursday the same week. Are two days enough to plan your trip? Perhaps it depends on many things, I had no reservations. The only one uncertainty was car parking logistics.
Those, who are familiar with Baltimore history and current life, know that your car is your Castle. After the Internet search and chats with my host family, the plan was to get a bus to NY which provides a designated car park.
Three hours on the bus flew in a flash. Wide roads with trees on both sides did remind me of some motorways in Russia. Gigantic tolls – almost 12 lanes in both directions. An impressive tunnel under the Hudson River connects the mainland with Manhatten.
An impressive tunnel under the Hudson River connects the mainland with Manhatten.  One can see a borderline dividing the tunnel into New Jersey and New York parts on about halfway.
One can see a borderline dividing the tunnel into New Jersey and New York parts on about halfway.
 What was my first impression of NY once I got off the bus? Many snapshots instantly jumped in linking with Hollywood movies that pictured NY. Mostly from ‘Sex and the City’. A traffic jam here and there. Crazy Taxi and car drivers. Brainless pedestrians. Everyone on the run. Madness. I did enjoy it as a tourist. Would I cope with it on everyday bases? A very big question!
What was my first impression of NY once I got off the bus? Many snapshots instantly jumped in linking with Hollywood movies that pictured NY. Mostly from ‘Sex and the City’. A traffic jam here and there. Crazy Taxi and car drivers. Brainless pedestrians. Everyone on the run. Madness. I did enjoy it as a tourist. Would I cope with it on everyday bases? A very big question!

Unfortunately, thanks to the hurricane Florence, not much sightseeing was on offer. All tall buildings were hidden with clouds. Tourists were queuing for hop-on-off.
 I had 2 hours before the bus to Baltimore. My choice was Times Square. A classical picture – huge screens are talking to you offering pleasure and entertainment. Come in, relax and enjoy!
I had 2 hours before the bus to Baltimore. My choice was Times Square. A classical picture – huge screens are talking to you offering pleasure and entertainment. Come in, relax and enjoy!
Strolling around Cafe shops, theaters, food vans. Looking at tourists and locals. Feeling and absorbing… Short, but sweet.
Christmas never ends at Times Square!

Many things to do next time…

Last year I have selected this photo of a lovely fountain capturing 3 girls under umbrellas (Drei-Mädchen-Brunnen) in Ballplatz Mainz in support of #ChildhoodCancerAwarnessMonth. This fountain was built between two Catholic girl’s schools symbolising the separate education and a happy childhood. It is charming on its own. And I’ve select it again.
Every child deserves a happy childhood. Raising awareness about childhood cancer we help to make the dreams of children with cancer come true. Dreams for a happy childhood, better treatment, better quality of life full of love ahead through better funding of childhood cancer research and access to innovative treatments.
Ok. This Monday is Labour Day – a public holiday celebrated on the 1st Monday in September in the US. According to the US Department of Labor, this holiday marks “a creation of the Labor movement and is dedicated to the social and economic achievements of American workers”. In contrast in Europe and Russia, it is celebrated on May 1st and known as May Day or International Workers’ Day and may or may not be a public holiday.
It is also the unofficial end of summer when many people arrange family gatherings or holidays. So, did our lab. We were all invited to our boss’ house to have a BBQ and chit-chat. As you may expect almost everyone in the lab has a multicultural background which is very proud of. You are in America, babe! I am not an exception. A proud Irish-Russian.

Everyone took advantage of and benefited from that mix. We had Mexican, Argentinian, French, Irish, Jewish, Ethiopian and American Indiana, Idaho, Florida, Maryland bites. Juicy steaks (raw, medium and well done) and burgers grilled by the host Andy were delicious. Have to admit that meat was tastier than I used to buy in Ireland. Should probably look for a new butcher when I come back!
What did surprise me the most? I have been thinking about it on the way home… None of 15 guests did check their mobile or take a pic of food/selfie during that time! Though everyone had this thing in the pocket. We were chatting and laughing. Maybe it is just that people… Fantastic company and a great day out.
Today marks the start of Childhood Cancer Awareness Month.
The cause of childhood cancers is believed to be due to faulty genes in stem cells that give rise to nerves, skin, blood and other body tissues. For some unknown reasons, the faulty genes can sit quiet and show their ‘bad’ character after birth and programme the cells into cancer cells.
So, there is no evidence that links lifestyle or environmental risk factors to the development of childhood cancer, which is opposite to many adult’s cancers.
Every 100th cancer patient is a child. Cancer is the 2nd most common cause of death among children after accidents.
Children are not little adults and so their cancer. Some childhood cancers have a good outlook and successful protocol of treatments. However, some of the cancers do not respond to the known drugs, or if respond cancer cells find the way to develop resistance and come back being more aggressive. Among theme are some forms of brain tumours, neuroblastoma and sarcomas; cancers developing in certain age groups and/or located within certain sites in the body, along with acute myeloid leukaemia (blood cancer). Children with a rare brain cancer – diffuse intrinsic pontine glioma survive less than 1 year from diagnosis. Children with soft tissue tumours have 5-year survival rates ranging from 64% (rhabdomyosarcoma) to 72% (Ewing sarcoma). Less than50% of children with the aggressive form of neuroblastoma will live beyond 5 years with current treatment strategies.
For majority of children who do survive cancer, the battle is never over. Over 60% of long‐term childhood cancer survivors have a chronic illness as a consequence of the treatment; over 25% have a severe or life-threatening illness.
The most common types of childhood cancer are:
Please see a short video The Childhood Cancer Ripple Effect created by St. Baldrick’s Foundation.